Department of Epidemiology, Johns Hopkins University, Baltimore, Maryland.
Department of Health Policy and Management, University of North Carolina, Chapel Hill.
JAMA Health Forum. 2022 Apr 15;3(4):e220575. doi: 10.1001/jamahealthforum.2022.0575. eCollection 2022 Apr.
Medicare accountable care organizations (ACOs) that disproportionately care for patients of racial and ethnic minority groups deliver lower quality care than those that do not, potentially owing to differences in out-of-network primary care among them.
To examine how organizational quality is associated with out-of-network primary care among ACOs that care for high vs low proportions of patients of racial and ethnic minority groups.
A retrospective cohort study was conducted between March 2019 and October 2021 using claims data (2013 to 2016) from a national sample of Medicare beneficiaries. Among beneficiaries who were assigned to 1 of 528 Medicare ACOs, a distinction was made between those treated by organizations that cared for high (vs low) proportions of patients of racial and ethnic minority groups. For each ACO, the amount of out-of-network primary care that it delivered annually was determined. Multivariable models were fit to evaluate how the quality of care that beneficiaries received varied by the proportion of care provided to patients of racial and ethnic minority groups by the ACO and its amount of out-of-network primary care.
The degree of care provided to patients of racial and ethnic minority groups by the ACO and its amount of out-of-network primary care.
The ACO quality assessed with 5 preventive care services and 4 utilization metrics.
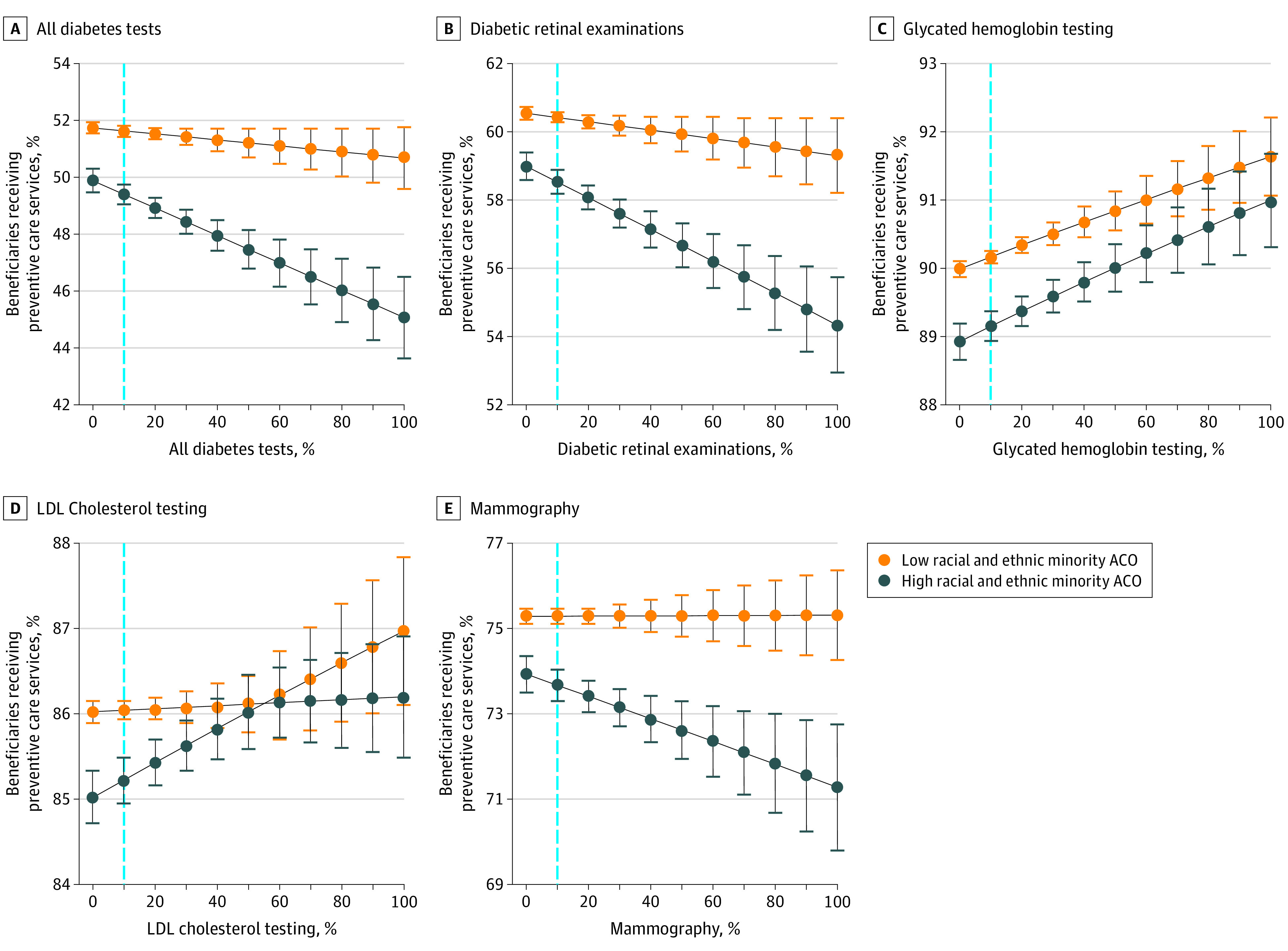
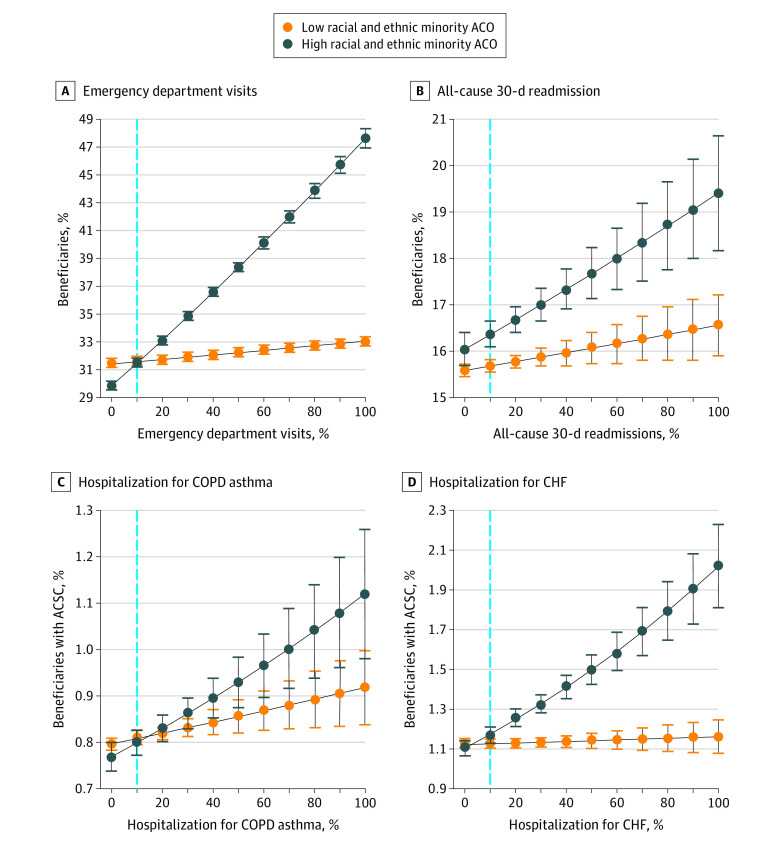
Among 3 955 951 beneficiary-years (2 320 429 [58.7%] women; 71 218 [1.8%] Asian, 267 684 [6.8%] Black, 44 059 [1.1%] Hispanic, 4922 [0.1%] North American Native, and 3 468 987 [87.7%] White individuals and 56 157 [1.4%] of Other race and ethnicity), those assigned to ACOs serving many patients of racial and ethnic minority groups at the mean level of out-of-network primary care were less likely than those assigned to ACOs serving fewer patients of racial and ethnic minority groups to receive diabetic retinal examinations (predicted probability, 49.4% [95%CI, 49.0%-49.7%] vs 51.6% [95% CI, 51.5%-51.8%]), glycated hemoglobin testing (predicted probability, 58.5% [95% CI, 58.2%-58.5%] vs 60.4% [95% CI, 60.3%-60.6%]), or low-density lipoprotein cholesterol testing (predicted probability, 85.2% [95% CI, 85.0%-85.5%] vs 86.0% [95% CI, 85.9%-86.1%]). They were also more likely to experience all-cause 30-day readmissions (predicted probability, 16.4% [95% CI, 16.1%-16.7%] vs 15.7% [95% CI, 15.6%-15.8%]). However, as the level of out-of-network primary care decreased, these gaps closed substantially, such that beneficiaries at ACOs that served many and fewer patients of racial and ethnic minority groups in the lowest percentile of out-of-network primary care received care of comparable quality.
This large cohort study found that quality performance among ACOs serving many patients of racial and ethnic minority groups was negatively associated with their level of out-of-network primary care.
重要性:不成比例地为少数族裔患者提供服务的医疗保险责任制医疗组织(ACO)的护理质量低于未提供此类服务的 ACO,这可能是由于它们之间的初级保健网络外服务存在差异。
目的:研究在为高比例(与低比例)少数族裔患者提供护理的 ACO 中,组织质量与 ACO 网络外初级保健之间的关系。
设计、地点和参与者:这是一项回顾性队列研究,于 2019 年 3 月至 2021 年 10 月期间,使用全国性的 Medicare 受益人群的索赔数据(2013 年至 2016 年)进行。在被分配到 528 个 Medicare ACO 中的受益人群中,将其分为由为高比例(与低比例)少数族裔患者提供护理的组织治疗的患者。对于每个 ACO,确定其每年提供的网络外初级保健量。使用多变量模型评估受益人群接受的护理质量如何随 ACO 为少数族裔患者提供的护理比例及其网络外初级保健量而变化。
暴露:ACO 为少数族裔患者提供的护理程度及其网络外初级保健量。
主要结果和措施:使用 5 项预防保健服务和 4 项利用指标评估 ACO 质量。
结果:在 3955951 个受益人群年(2320429 名女性[58.7%];71218 名亚洲人[1.8%],267684 名黑人[6.8%],44059 名西班牙裔[1.1%],4922 名北美原住民[0.1%]和 3468987 名白人[87.7%]和 36157 名其他种族[1.4%])中,与为少数族裔患者提供服务较少的 ACO 相比,为服务较多的 ACO 分配的人群接受糖尿病视网膜检查的可能性较低(预测概率,49.4%[95%CI,49.0%-49.7%]与 51.6%[95%CI,51.5%-51.8%]),糖化血红蛋白检测(预测概率,58.5%[95%CI,58.2%-58.5%]与 60.4%[95%CI,60.3%-60.6%])或低密度脂蛋白胆固醇检测(预测概率,85.2%[95%CI,85.0%-85.5%]与 86.0%[95%CI,85.9%-86.1%])的可能性较低。他们还更有可能经历所有原因的 30 天再入院(预测概率,16.4%[95%CI,16.1%-16.7%]与 15.7%[95%CI,15.6%-15.8%])。然而,随着网络外初级保健量的减少,这些差距大大缩小,以至于在网络外初级保健量最低的 ACO 中,为服务较多和较少的少数族裔患者提供护理的人群获得了质量相当的护理。
结论和相关性:这项大型队列研究发现,为大量少数族裔患者提供服务的 ACO 的服务质量与他们的网络外初级保健水平呈负相关。