First Department of Cardiology, Interventional Electrocardiology and Hypertension, Jagiellonian University, Medical College, Jakubowskiego 2, 30-688 Krakow, Poland.
Electrophysiology Section, Cardiology Department, Hospital Universitari i Politècnic La Fe, Valencia, Spain.
Eur Heart J. 2022 Oct 21;43(40):4161-4173. doi: 10.1093/eurheartj/ehac445.
Permanent transseptal left bundle branch area pacing (LBBAP) is a promising new pacing method for both bradyarrhythmia and heart failure indications. However, data regarding safety, feasibility and capture type are limited to relatively small, usually single centre studies. In this large multicentre international collaboration, outcomes of LBBAP were evaluated.
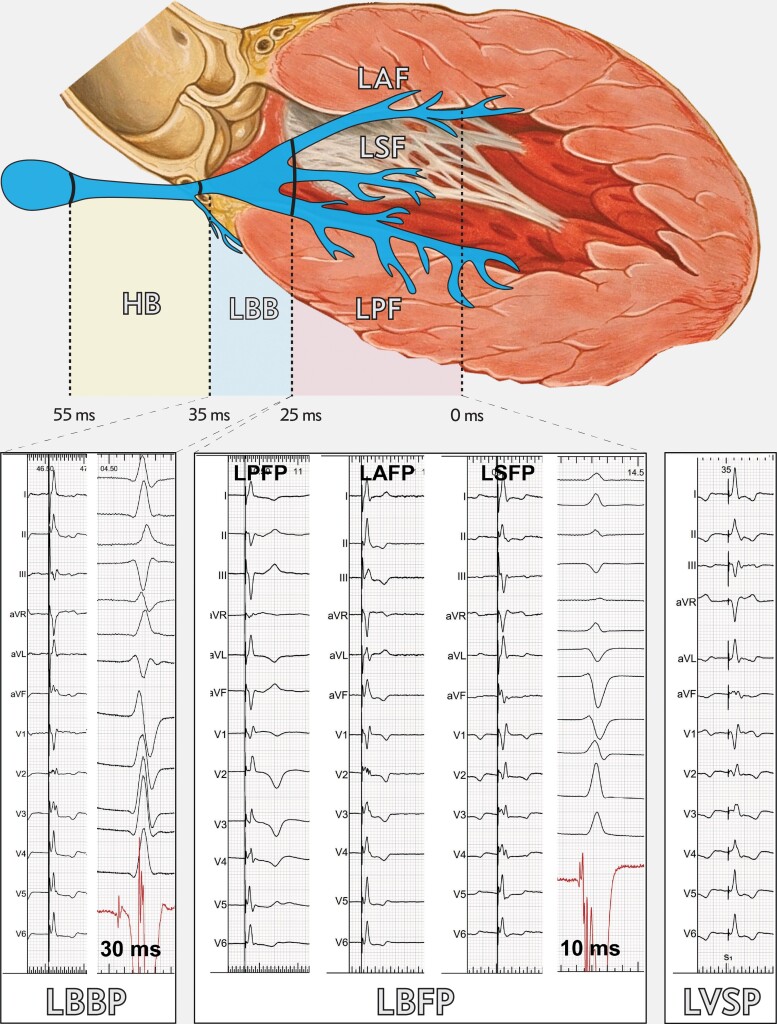
This is a registry-based observational study that included patients in whom LBBAP device implantation was attempted at 14 European centres, for any indication. The study comprised 2533 patients (mean age 73.9 years, female 57.6%, heart failure 27.5%). LBBAP lead implantation success rate for bradyarrhythmia and heart failure indications was 92.4% and 82.2%, respectively. The learning curve was steepest for the initial 110 cases and plateaued after 250 cases. Independent predictors of LBBAP lead implantation failure were heart failure, broad baseline QRS and left ventricular end-diastolic diameter. The predominant LBBAP capture type was left bundle fascicular capture (69.5%), followed by left ventricular septal capture (21.5%) and proximal left bundle branch capture (9%). Capture threshold (0.77 V) and sensing (10.6 mV) were stable during mean follow-up of 6.4 months. The complication rate was 11.7%. Complications specific to the ventricular transseptal route of the pacing lead occurred in 209 patients (8.3%).
LBBAP is feasible as a primary pacing technique for both bradyarrhythmia and heart failure indications. Success rate in heart failure patients and safety need to be improved. For wider use of LBBAP, randomized trials are necessary to assess clinical outcomes.
永久性左束支区域起搏(LBBAP)是一种有前途的新起搏方法,适用于心动过缓和心力衰竭等适应证。然而,关于安全性、可行性和夺获类型的数据仅限于相对较小的、通常是单中心的研究。在这项大型多中心国际合作中,评估了 LBBAP 的结果。
这是一项基于注册的观察性研究,纳入了 14 个欧洲中心因任何适应证而尝试进行 LBBAP 装置植入的患者。该研究包括 2533 例患者(平均年龄 73.9 岁,女性占 57.6%,心力衰竭占 27.5%)。LBBAP 导联植入术用于心动过缓和心力衰竭适应证的成功率分别为 92.4%和 82.2%。学习曲线在最初的 110 例中最为陡峭,在 250 例后趋于平稳。LBBAP 导联植入失败的独立预测因素有心衰、宽基线 QRS 和左心室舒张末期直径。LBBAP 夺获的主要类型为左束支纤维束夺获(69.5%),其次为左心室间隔夺获(21.5%)和左束支近端夺获(9%)。在平均 6.4 个月的随访中,夺获阈值(0.77 V)和感知(10.6 mV)保持稳定。并发症发生率为 11.7%。与心室经间隔起搏导联相关的并发症发生在 209 例患者(8.3%)中。
LBBAP 作为心动过缓和心力衰竭等适应证的主要起搏技术是可行的。需要提高心力衰竭患者的成功率和安全性。为了更广泛地使用 LBBAP,需要进行随机试验来评估临床结果。