Center for Aging in Diverse Communities, University of California, San Francisco, San Francisco.
Multiethnic Health Equity Research Center, Division of General Internal Medicine, Department of Medicine, University of California, San Francisco, San Francisco.
JAMA Netw Open. 2022 Aug 1;5(8):e2227658. doi: 10.1001/jamanetworkopen.2022.27658.
Depression is a debilitating and costly medical condition that is often undertreated. Men, racial and ethnic minority individuals, older adults, and those with language barriers are at increased risk for undertreatment of depression. Disparities in screening may contribute to undertreatment.
To examine depression screening rates among populations at risk for undertreatment of depression during and after rollout of general screening.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study from September 1, 2017, to December 31, 2019, of electronic health record data from 52 944 adult patients at 6 University of California, San Francisco, primary care facilities assessed depression screening rates after implementation of a general screening policy. Patients were excluded if they had a baseline diagnosis of depression, bipolar disorder, schizophrenia, schizoaffective disorder, or dementia.
Screening year, including rollout (September 1, 2017, to December 31, 2017) and each subsequent calendar year (January 1 to December 31, 2018, and January 1 to December 31, 2019).
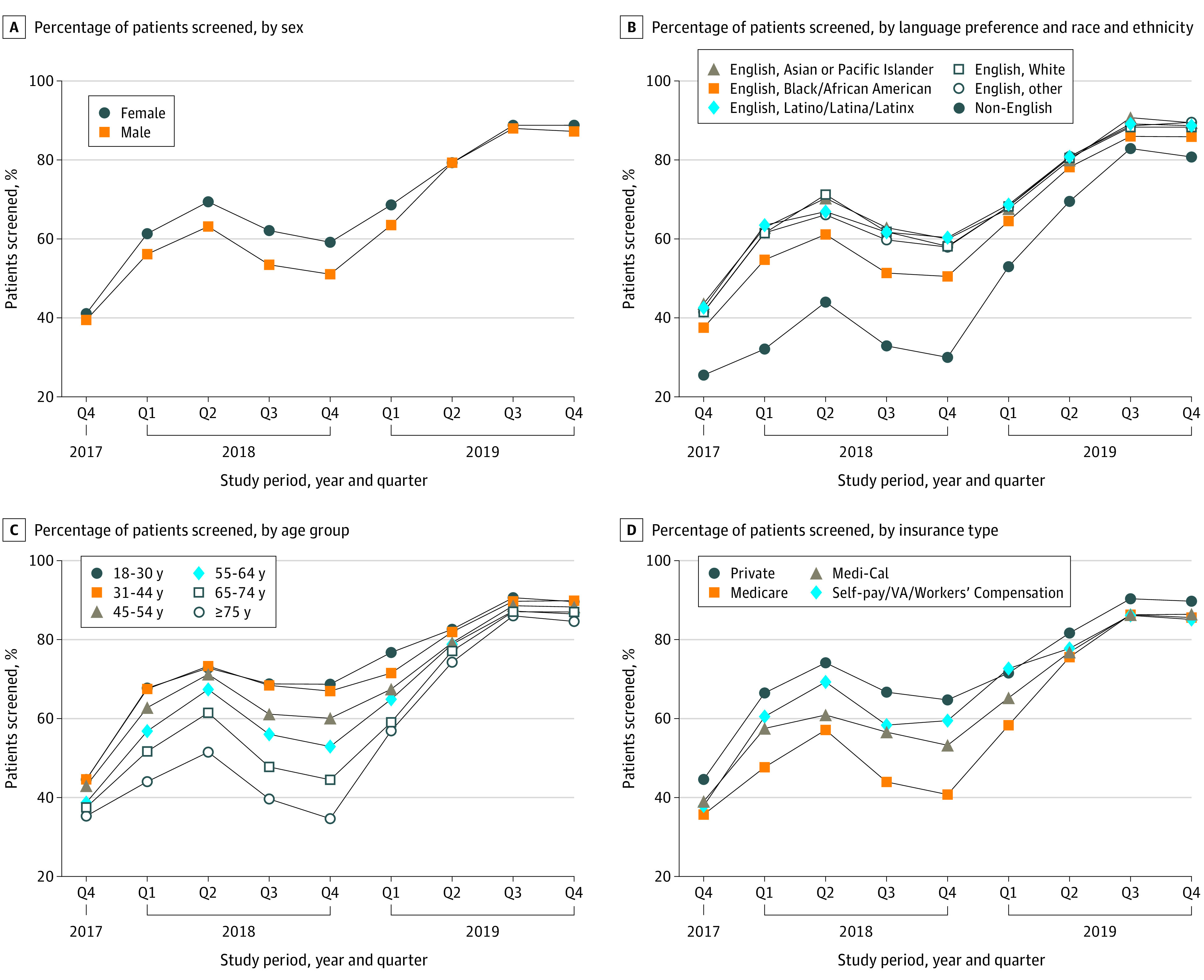
Rates of depression screening performed by medical assistants using the Patient Health Questionnaire-2. Data collected included age, sex, race and ethnicity, and language preference (English vs non-English); to compare English and non-English language preference groups and also assess depression screening by race and ethnicity within the English-speaking group, a single language-race-ethnicity variable with non-English language preference and English language preference categories was created. In multivariable analyses, the likelihood of being screened was evaluated using annual logistic regression models for 2018 and 2019, examining sex, age, language-race-ethnicity, and comorbidities, with adjustment for primary care site.
There were 52 944 unique, eligible patients with 1 or more visits in one of the 6 primary care practices during the entire study period (59% female; mean [SD] age, 48.9 [17.6] years; 178 [0.3%] American Indian/Alaska Native, 13 241 [25.0%] English-speaking Asian, 3588 [6.8%] English-speaking Black/African American, 4744 [9.0%] English-speaking Latino/Latina/Latinx, 760 [1.4%] Pacific Islander, 22 689 [42.9%] English-speaking White, 4857 [9.0%] English-speaking other [including individuals who indicated race and ethnicity as other and individuals for whom race and ethnicity data were missing or unknown], and 2887 [5.5%] with language barriers [non-English language preference]). Depression screening increased from 40.5% at rollout (2017) to 88.8% (2019). In 2018, the likelihood of being screened decreased with increasing age (adusted odds ratio [aOR], 0.89 [95% CI, 0.82-0.98] for ages 45-54 and aOR, 0.75 [95% CI, 0.65-0.85] for ages 75 and older compared with ages 18-30); and, except for Spanish-speaking patients, patients with limited English proficiency were less likely to be screened for depression than English-speaking White patients (Chinese language preference: aOR, 0.59 [95% CI, 0.51-0.67]; other non-English language preference: aOR, 0.55 [95% CI, 0.47-0.64]). By 2019, depression screening had increased dramatically for all at-risk groups, and for most, disparities had disappeared; the odds of screening were only still significantly lower for men compared with women (aOR, 0.87 [95% CI, 0.81 to 0.93]).
In this cohort study in a large academic health system, full implementation of depression screening was associated with a substantial increase in screening rates among groups at risk for undertreatment of depression. In addition, depression screening disparities narrowed over time for most groups, suggesting that routine depression screening in primary care may reduce screening disparities and improve recognition and appropriate treatment of depression for all patients.
抑郁症是一种使人衰弱且代价高昂的医疗状况,往往治疗不足。男性、少数族裔、老年人以及存在语言障碍的人患抑郁症治疗不足的风险增加。筛查方面的差异可能导致治疗不足。
在普遍筛查推出期间和之后,调查在抑郁症治疗不足风险人群中进行抑郁症筛查的比例。
设计、地点和参与者:本队列研究于 2017 年 9 月 1 日至 2019 年 12 月 31 日,从加利福尼亚大学旧金山分校的 6 个初级保健机构的 52944 名成年患者的电子健康记录数据中评估实施普遍筛查政策后抑郁症筛查率。如果患者基线诊断为抑郁症、双相情感障碍、精神分裂症、分裂情感性障碍或痴呆,则将其排除在外。
筛查年份,包括推出年份(2017 年 9 月 1 日至 2017 年 12 月 31 日)和随后的每个历年(2018 年 1 月 1 日至 2018 年 12 月 31 日和 2019 年 1 月 1 日至 2019 年 12 月 31 日)。
医疗助理使用患者健康问卷-2 进行抑郁症筛查的比例。收集的数据包括年龄、性别、种族和族裔以及语言偏好(英语与非英语);为了比较英语和非英语语言偏好群体,并评估英语语言群体中的种族和族裔抑郁症筛查情况,创建了一个包含非英语语言偏好和英语语言偏好类别的单一语言-种族-族裔变量。在多变量分析中,使用 2018 年和 2019 年的年度逻辑回归模型评估被筛查的可能性,检查性别、年龄、语言-种族-族裔以及合并症,并根据初级保健地点进行调整。
在整个研究期间,有 52944 名具有独特合格就诊记录的患者在 6 个初级保健机构中的一个机构就诊过 1 次或多次(59%为女性;平均[标准差]年龄为 48.9[17.6]岁;178[0.3%]美国印第安人/阿拉斯加原住民,13241[25.0%]讲英语的亚裔,3588[6.8%]讲英语的非裔美国人,4744[9.0%]讲英语的拉丁裔/拉丁裔/拉丁裔,760[1.4%]太平洋岛民,22689[42.9%]讲英语的白人,4857[9.0%]讲英语的其他种族[包括将种族和族裔表示为其他的个体和种族和族裔数据缺失或未知的个体],2887[5.5%]有语言障碍[非英语语言偏好])。抑郁症筛查率从推出时的 40.5%(2017 年)增加到 88.8%(2019 年)。在 2018 年,被筛查的可能性随着年龄的增长而降低(年龄在 45-54 岁的调整优势比[aOR]为 0.89[95%CI,0.82-0.98],年龄在 75 岁及以上的 aOR 为 0.75[95%CI,0.65-0.85],与 18-30 岁的年龄相比);除了讲西班牙语的患者外,与讲英语的白人患者相比,英语水平有限的患者进行抑郁症筛查的可能性较小(讲中文的偏好:aOR,0.59[95%CI,0.51-0.67];其他非英语语言偏好:aOR,0.55[95%CI,0.47-0.64])。到 2019 年,所有高风险群体的抑郁症筛查率都大幅增加,而且对于大多数群体来说,差异已经消失;与女性相比,男性的筛查几率仍然明显较低(aOR,0.87[95%CI,0.81 至 0.93])。
在这项针对大型学术医疗系统中大量成年患者的队列研究中,抑郁症筛查的全面实施与治疗不足风险人群中筛查率的大幅增加有关。此外,随着时间的推移,大多数群体的抑郁症筛查差异缩小,这表明在初级保健中常规进行抑郁症筛查可能会减少筛查差异,并改善所有患者对抑郁症的识别和适当治疗。