Haase Lucas, Wise Kelsey, Kelly Brandon, Harris John, Macalena Jeffrey
Orthopedic Surgery, University Hospitals Cleveland Medical Center, Cleveland, USA.
Orthopedic Surgery, University of Minnesota, Minneapolus, USA.
Cureus. 2022 Jul 18;14(7):e26988. doi: 10.7759/cureus.26988. eCollection 2022 Jul.
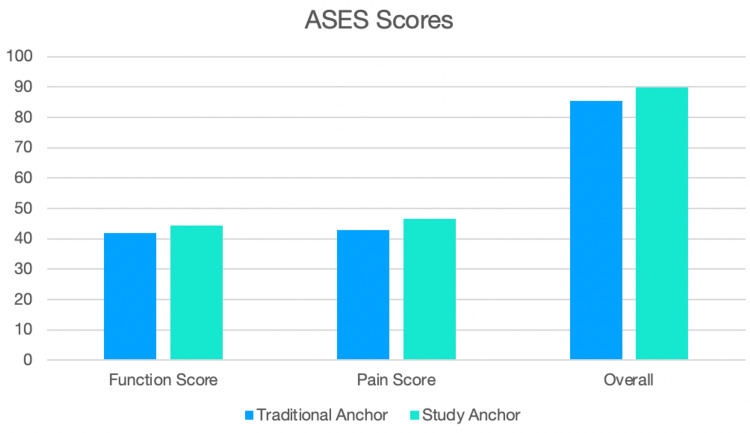
Background Shoulder instability and recurrent dislocations are common problems encountered by orthopedic surgeons and are frequently associated with a Bankart lesion. These are classically treated with either open or arthroscopic repair utilizing traditional suture anchors, though anchorless fixation techniques have recently been developed as an alternate fixation method that reduces native bone loss and has comparable pull-out strength. Methods A retrospective review was performed at a single institution for patients who underwent Bankart repair from January 2008 through February 2014. American Shoulder and Elbow Surgeons (ASES) questionnaires were mailed to 35 patients with anchorless fixation and 35 age-, gender-, and surgeon-matched patients with traditional suture anchors. Statistical analysis was performed comparing re-dislocation, additional surgery, and ASES scores with statistical significance set at p < 0.05. Results Eleven patients in the anchorless implant group and 15 patients in the anchor group completed the questionnaire. The mean follow-up was 4.1 years in the anchorless group and 5.6 years in the anchor group (p=0.04). The number of implants was 4.82 in the anchorless group and 3.87 in the anchor group (p = 0.04). No difference was found in re-dislocation rates (p = 0.80) or additional surgery on the affected shoulder (p = 0.75). ASES scores were found to have no statistical difference (89.89 for the anchorless group versus 85.37 for the anchor group; p = 0.78). Conclusion In patients undergoing arthroscopic Bankart lesion repair with traditional anchors compared to anchorless fixation, there appears to be no difference in shoulder re-dislocation rates, recurrent ipsilateral shoulder surgery, or ASES scores.
肩部不稳定和复发性脱位是骨科医生常见的问题,且常与Bankart损伤相关。传统上,这些损伤通过使用传统缝线锚钉进行开放或关节镜修复来治疗,不过最近已开发出无锚钉固定技术作为一种替代固定方法,该方法可减少自体骨丢失且具有相当的拔出强度。
在一家机构对2008年1月至2014年2月期间接受Bankart修复的患者进行回顾性研究。向35例接受无锚钉固定的患者和35例年龄、性别及手术医生匹配的接受传统缝线锚钉治疗的患者邮寄美国肩肘外科医师学会(ASES)问卷。进行统计分析以比较再脱位、额外手术及ASES评分,设定p<0.05为具有统计学意义。
无锚钉植入组11例患者和锚钉组15例患者完成了问卷。无锚钉组的平均随访时间为4.1年,锚钉组为5.6年(p = 0.04)。无锚钉组的植入物数量为4.82个,锚钉组为3.87个(p = 0.04)。再脱位率(p = 0.80)或患侧肩部的额外手术(p = 0.75)方面未发现差异。发现ASES评分无统计学差异(无锚钉组为89.89,锚钉组为85.37;p = 0.78)。
与无锚钉固定相比,在接受传统锚钉进行关节镜下Bankart损伤修复的患者中,肩部再脱位率、同侧肩部复发性手术或ASES评分似乎没有差异。