Tang Zhiji, Hu Kun, Yang Ruijin, Zou Mingang, Zhong Ming, Huang Qiangliang, Wei Wenjin, Jiang Qiuhua
Department of Neurosurgery, Ganzhou People's Hospital, Ganzhou, China.
Department of Neurosurgery, HuiChang County People's Hospital, HuiChang, China.
Front Neurol. 2022 Aug 3;13:944608. doi: 10.3389/fneur.2022.944608. eCollection 2022.
This study was designed to develop and validate a risk-prediction nomogram to predict a 6-month unfavorable prognosis in patients with traumatic brain-injured (TBI) undergoing primary decompressive craniectomy (DC).
The clinical data of 391 TBI patients with primary DC who were admitted from 2012 to 2020 were reviewed, from which 274 patients were enrolled in the training group, while 117 were enrolled in the internal validation group, randomly. The external data sets containing 80 patients were obtained from another hospital. Independent predictors of the 6-month unfavorable prognosis were analyzed using multivariate logistic regression. Furthermore, a nomogram prediction model was constructed using R software. After evaluation of the model, internal and external validations were performed to verify the efficiency of the model using the area under the receiver operating characteristic curves and the calibration plots.
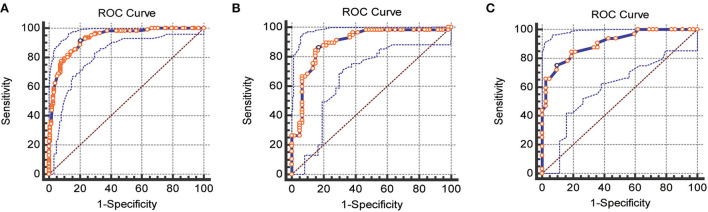
In multivariate analysis, age( = 0.001), Glasgow Score Scale (GCS) ( < 0.001), operative blood loss of >750 ml ( = 0.045), completely effaced basal cisterns ( < 0.001), intraoperative hypotension( = 0.001), and activated partial thromboplastin time (APTT) of >36 ( = 0.012) were the early independent predictors for 6-month unfavorable prognosis in patients with TBI after primary DC. The AUC for the training, internal, and external validation cohorts was 0.93 (95%CI, 0.89-0.96, < 0.0001), 0.89 (95%CI, 0.82-0.94, < 0.0001), and 0.90 (95%CI, 0.84-0.97, < 0.0001), respectively, which indicated that the prediction model had an excellent capability of discrimination. Calibration of the model was exhibited by the calibration plots, which showed an optimal concordance between the predicted 6-month unfavorable prognosis probability and actual probability in both training and validation cohorts.
This prediction model for a 6-month unfavorable prognosis in patients with TBI undergoing primary DC can evaluate the prognosis accurately and enhance the early identification of high-risk patients.
本研究旨在开发并验证一种风险预测列线图,以预测接受初次减压颅骨切除术(DC)的创伤性脑损伤(TBI)患者6个月时的不良预后。
回顾了2012年至2020年收治的391例行初次DC的TBI患者的临床资料,其中274例患者被纳入训练组,117例患者被随机纳入内部验证组。另外从另一家医院获取了包含80例患者的外部数据集。使用多因素逻辑回归分析6个月不良预后的独立预测因素。此外,使用R软件构建列线图预测模型。对模型进行评估后,使用受试者操作特征曲线下面积和校准图进行内部和外部验证,以验证模型的有效性。
在多因素分析中,年龄(P = 0.001)、格拉斯哥昏迷量表(GCS)评分(P < 0.001)、术中失血量>750 ml(P = 0.045)、基底池完全消失(P < 0.001)、术中低血压(P = 0.001)以及活化部分凝血活酶时间(APTT)>36(P = 0.012)是初次DC后TBI患者6个月不良预后的早期独立预测因素。训练组、内部验证组和外部验证组的曲线下面积(AUC)分别为0.93(95%CI,0.89 - 0.96,P < 0.0001)、0.89(95%CI,0.82 - 0.94,P < 0.0001)和0.90(95%CI,0.84 - 0.97,P < 0.0001),这表明预测模型具有出色的区分能力。校准图显示了模型的校准情况,表明在训练组和验证组中,预测的6个月不良预后概率与实际概率之间具有最佳一致性。
这种用于预测接受初次DC的TBI患者6个月不良预后的预测模型能够准确评估预后,并加强对高危患者的早期识别。