School of Psychology, Cardiff University, Cardiff, UK.
Instituto Superior Miguel Torga, Coimbra, Portugal.
Hum Reprod. 2022 Sep 30;37(10):2412-2425. doi: 10.1093/humrep/deac168.
Is it feasible to implement and evaluate an online self-guided psychosocial intervention for people with an unmet parenthood goal (UPG), aimed to improve well-being, in an online randomized controlled trial (RCT)?
The evaluation of an online bilingual self-guided psychosocial intervention for people with a UPG is feasible, reflected by high demand, good acceptability, good adaptation and promise of efficacy, but minor adjustments to the intervention and study design of the RCT should be made to enhance practicality.
Self-identifying as having a UPG, defined as being unable to have children or as many as desired, is associated with impaired well-being and mental health. Practice guidelines and regulatory bodies have highlighted the need to address the lack of evidence-based support for this population. It is unknown if MyJourney (www.myjourney.pt), the first online self-guided intervention for people with UPGs, can be implemented and evaluated in an RCT.
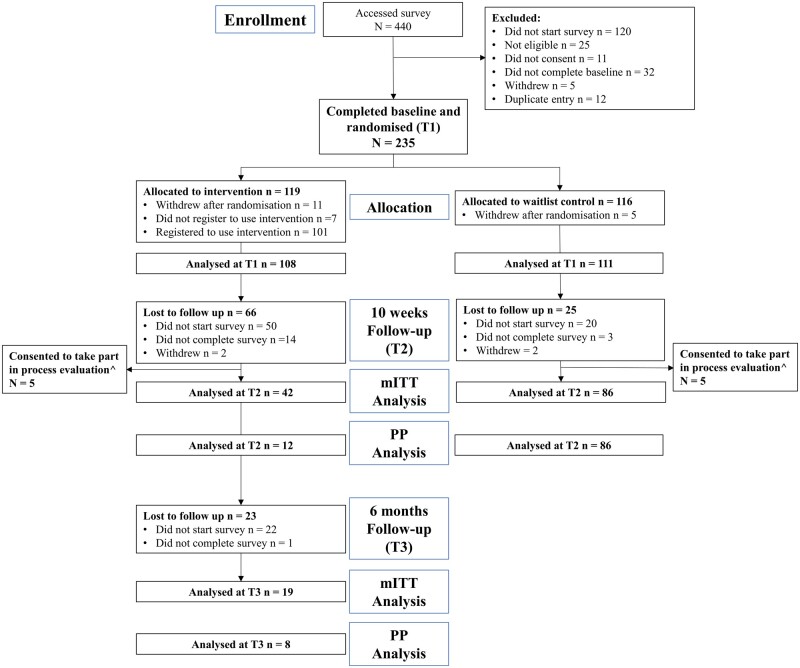
STUDY DESIGN, SIZE, DURATION: To evaluate the feasibility of MyJourney, we conducted a registered, two-arm, parallel group, non-blinded feasibility RCT, with a 1:1 computer-generated randomized allocation and embedded qualitative process evaluation. Participants were included between November 2020 and March 2021. Assessments were made before randomization (T1), 10 weeks (T2) and 6 months after (T3, intervention group only). Participants allocated to the intervention group received an email to access MyJourney immediately after randomization. Participants in the waitlist control group were given access to MyJourney after completing the 10-week assessment (T2).
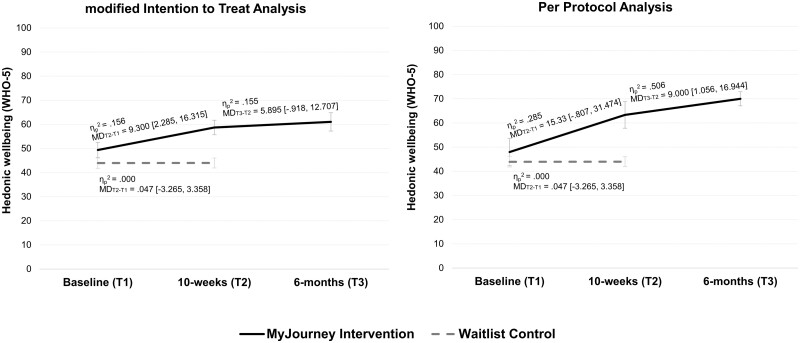
PARTICIPANTS/MATERIALS, SETTING, METHODS: Participants were recruited via social media advertising of MyJourney and its feasibility study. People who self-identified as having a UPG could click on a link to participate, and of these 235 were randomized. Outcome measures related to demand, acceptability, implementation, practicality, adaptation and limited efficacy were assessed via online surveys. The primary outcome in limited efficacy testing was hedonic well-being, measured with the World Health Organisation Wellbeing Index (WHO-5).
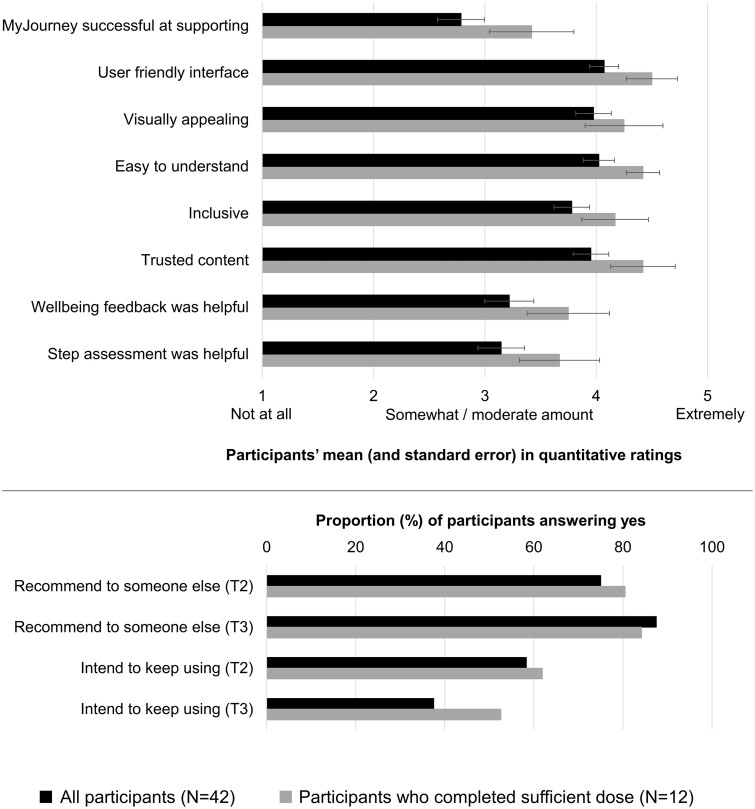
Participation and retention rates were 58.3%, 31.7% (T2) and 45.2% (T3, intervention group only), respectively. Of participants invited to register with MyJourney, 91 (76.5%) set up an account, 51 (47.2%) completed the first Step of MyJourney, 12 (11.1%) completed six Steps (sufficient dose) and 6 (5.6%) completed all Steps within the 10-week recommended period. Acceptability ranged from 2.79 (successful at supporting) to 4.42 (easy to understand) on a 1 (not at all) to 5 (extremely acceptable) scale. Average time to complete sufficient dose was 15.6 h (SD = 18.15) and to complete all Steps was 12.4 h (SD = 18.15), with no differences found for participants using MyJourney in Portuguese and English. Modified intention-to-treat analysis showed a moderate increase in well-being from T1 to T2 in the intervention group (ηp2 = 0.156, mean difference (MD) = 9.300 (2.285, 16.315)) and no changes in the control group (ηp2 = 0.000, MD = 0.047 (-3.265, 3.358)). Participants in the process evaluation reported MyJourney was needed and answered their needs for support (reflecting high demand and acceptability), the recommended period to engage with MyJourney was short, and their engagement was influenced by multiple factors, including personal (e.g. lack of time) and MyJourney related (e.g. reminders).
LIMITATIONS, REASONS FOR CAUTION: Participants were mostly white, well-educated, employed, childless women. Non-blinded allocation, use of self-reported questionnaire assessments and high attrition in the intervention group could have triggered bias favourable to positive evaluations of MyJourney and resulted in low power to detect T2 to T3 changes in limited efficacy outcomes.
MyJourney can proceed to efficacy testing, but future work should eliminate barriers for engagement and explore strategies to maximize adherence. Entities wanting to support people with UPGs now have a freely accessible and promising resource that can be further tested and evaluated in different settings.
STUDY FUNDING/COMPETING INTEREST(S): MyJourney's development was funded by the charity Portuguese Fertility Association, Cardiff University and University of Coimbra (CINEICC). Dr S.G. reports consultancy fees from Ferring Pharmaceuticals A/S, speaker fees from Access Fertility, SONA-Pharm LLC, Meridiano Congress International and Gedeon Richter and grants from Merck Serono Ltd. Bethan Rowbottom holds a PhD scholarship funded by the School of Psychology, Cardiff University. The other authors have no conflicts of interest.
Clinical Trials.gov NCT04850482.
在一项在线随机对照试验 (RCT) 中,实施和评估针对未满足育儿目标 (UPG) 的人群的在线自我指导心理社会干预措施以提高幸福感是否可行?
评估针对 UPG 人群的双语在线自我指导心理社会干预措施是可行的,这反映在高需求、良好的可接受性、良好的适应性和疗效的潜力上,但干预措施和 RCT 的研究设计应进行一些小的调整,以提高实用性。
自我认定为 UPG,定义为无法生育或想要的孩子数量不足,与幸福感和心理健康受损有关。实践指南和监管机构强调需要解决针对这一人群缺乏循证支持的问题。目前尚不清楚第一个针对 UPG 人群的在线自我指导干预措施 MyJourney 是否可以在 RCT 中实施和评估。
研究设计、规模、持续时间:为了评估 MyJourney 的可行性,我们进行了一项已注册的、两臂、平行组、非盲法可行性 RCT,采用 1:1 计算机生成的随机分配和嵌入式定性过程评估。参与者于 2020 年 11 月至 2021 年 3 月期间入选。在随机分组前 (T1)、10 周 (T2) 和 6 个月后 (仅干预组的 T3) 进行评估。随机分组后立即向干预组的参与者发送电子邮件以访问 MyJourney。等待对照组的参与者在完成 10 周评估 (T2) 后可访问 MyJourney。
参与者/材料、地点、方法:通过 MyJourney 及其可行性研究的社交媒体广告招募参与者。自我认定为 UPG 的人可以点击链接参与,其中 235 人被随机分组。通过在线调查评估与需求、可接受性、实施、实用性、适应性和有限疗效相关的措施。有限疗效测试的主要结果是幸福感,使用世界卫生组织幸福感指数 (WHO-5) 进行衡量。
参与率和保留率分别为 58.3%、31.7%(T2)和 45.2%(仅干预组的 T3)。邀请注册 MyJourney 的参与者中,91 人(76.5%)注册了账户,51 人(47.2%)完成了 MyJourney 的第一步,12 人(11.1%)完成了六个步骤(足够剂量),6 人(5.6%)在建议的 10 周内完成了所有步骤。可接受性在 2.79(成功支持)到 4.42(易于理解)之间,满分 1(完全不可接受)到 5(非常可接受)。完成足够剂量的平均时间为 15.6 小时(SD=18.15),完成所有步骤的平均时间为 12.4 小时(SD=18.15),使用葡萄牙语和英语的参与者之间没有差异。修改后的意向治疗分析显示,干预组的幸福感从 T1 到 T2 中度增加(ηp2=0.156,MD=9.300(2.285,16.315)),对照组没有变化(ηp2=0.000,MD=0.047(-3.265,3.358))。过程评估中的参与者报告说 MyJourney 是必要的,满足了他们的支持需求(反映了高需求和可接受性),与 MyJourney 互动的推荐时间很短,他们的参与受到多种因素的影响,包括个人因素(例如时间不足)和与 MyJourney 相关的因素(例如提醒)。
局限性、谨慎的原因:参与者主要是白人、受过良好教育、有工作、没有孩子的女性。非盲分配、使用自我报告的问卷调查评估以及干预组的高失访率可能会引发有利于 MyJourney 积极评价的偏差,并导致有限疗效结果的 T2 到 T3 变化的检测能力较低。
MyJourney 可以进行疗效测试,但未来的工作应消除参与障碍,并探索提高依从性的策略。希望支持 UPG 人群的实体现在有了一个免费的、有前途的资源,可以在不同的环境中进一步测试和评估。
研究资金/利益冲突:MyJourney 的开发得到了葡萄牙生育协会、卡迪夫大学和科英布拉大学(CINEICC)的慈善机构的资助。S.G. 博士报告了与 Ferring 制药公司、Access Fertility、SONA-Pharm LLC、Meridiano Congress International 和 Gedeon Richter 的咨询费,以及 Merck Serono Ltd. 的资助。Bethan Rowbottom 持有卡迪夫大学心理学系的博士奖学金。其他作者没有利益冲突。
ClinicalTrials.gov NCT04850482。