iEH2 (Institute for Ethics, History and the Humanities), Faculty of Medicine, University of Geneva, Geneva, Switzerland.
Department of Information Science, Geneva School of Business Administration, Geneva, Switzerland.
BMC Med Ethics. 2022 Aug 24;23(1):86. doi: 10.1186/s12910-022-00815-7.
Implicit prejudice can lead to disparities in treatment. The effects of specialty and experience on implicit obesity and mental illness prejudice had not been explored. The main objective was to examine how specializing in psychiatry/general medicine and years of experience moderated implicit obesity and mental illness prejudice among Swiss physicians. Secondary outcomes included examining the malleability of implicit bias via two video interventions and a condition of cognitive load, correlations of implicit bias with responses to a clinical vignette, and correlations with explicit prejudice.
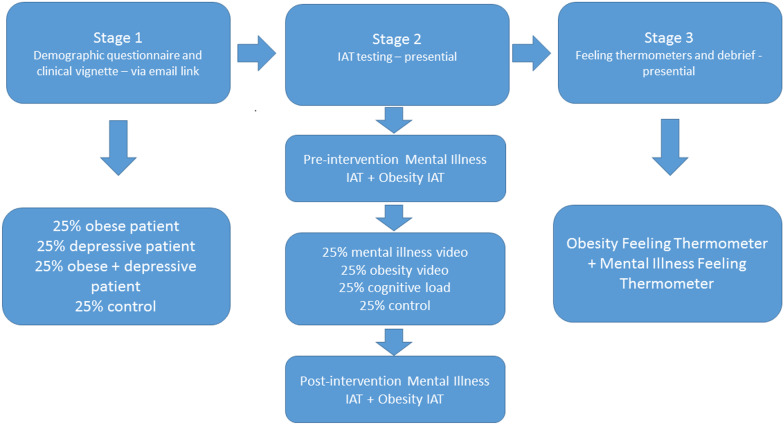
In stage 1, participants completed an online questionnaire including a clinical vignette. In stage 2, implicit prejudice pre- and post- intervention was tested using a 4 × 4 between-subject design including a control group. In stage 3, explicit prejudice was tested with feeling thermometers and participants were debriefed. Participants were 133 psychiatrists and internists working in Geneva, hospital-based and private practice. Implicit prejudice was assessed using a Weight IAT (Implicit Association Test) and a Mental Illness IAT. Explicit feelings towards the obese and the mentally ill were measured using Feeling Thermometers. A clinical vignette assessed the level of concern felt for a fictional patient under four conditions: control, obese, depression, obese and depression. Linear regression was conducted to test for association of gender, experience, and specialty with responses to vignettes, pre-intervention IATs and explicit attitudes, and to test for association of interventions (or control) with post-intervention IATs and explicit attitudes. Reported effect sizes were computed using Cohen's d. Two-tailed p < 0.05 was selected as the significance threshold.
Compared to internists, psychiatrists showed significantly less implicit bias against mentally vs. physically ill people than internists and warmer explicit feelings towards the mentally ill. More experienced physicians displayed warmer explicit feelings towards the mentally ill and a greater level of concern for the fictional patients in the vignette than the less experienced, except when the patient was described as obese.
Specialty moderates both implicit and explicit mental illness prejudice. Experience moderates explicit mental illness bias and concern for patients. The effect of specialty on implicit prejudice seems to be based principally on self-selection.
内隐偏见可能导致治疗上的差异。专业和经验对肥胖和精神疾病内隐偏见的影响尚未得到探讨。主要目的是研究瑞士医生在精神病学/普通医学专业方面的专长和经验年限如何调节对肥胖和精神疾病的内隐偏见。次要结果包括通过两个视频干预和认知负荷条件来检查内隐偏差的可塑程度,内隐偏差与临床病例的相关性,以及与外显偏见的相关性。
在第 1 阶段,参与者完成了一项在线问卷调查,包括一个临床病例。在第 2 阶段,通过包括对照组的 4×4 被试间设计,使用肥胖 IAT(内隐联想测验)和精神疾病 IAT 测试干预前后的内隐偏见。在第 3 阶段,使用情感温度计测试外显偏见,并对参与者进行汇报。参与者是在日内瓦工作的精神病医生和内科医生,包括医院和私人诊所。使用体重 IAT(内隐联想测验)和精神疾病 IAT 评估内隐偏见。使用情感温度计测量对肥胖和精神疾病患者的明确感受。一个临床病例评估了在四种情况下对虚构患者的关注程度:控制、肥胖、抑郁、肥胖和抑郁。进行线性回归以测试性别、经验和专业与病例反应、干预前 IAT 和外显态度的相关性,并测试干预(或控制)与干预后 IAT 和外显态度的相关性。报告的效应大小使用 Cohen's d 计算。选择双侧 p<0.05 作为显著性阈值。
与内科医生相比,精神病医生对精神疾病患者的内隐偏见明显低于内科医生,对外科医生的外显感受更温暖。经验丰富的医生对外科医生的精神疾病患者的外显感受更温暖,对病例中虚构患者的关注程度也更高,除了患者被描述为肥胖时。
专业调节内隐和外显的精神疾病偏见。经验调节对外科医生的精神疾病偏见和对患者的关注。专业对内隐偏见的影响似乎主要基于自我选择。