Qiu Yuwei, Gu Wei, Zhao Mingye, Zhang Yunyun, Wu Jingxiang
Department of Anesthesiology, Shanghai Chest Hospital, Shanghai Jiao Tong University, Shanghai, China.
Outcomes Research Consortium, Cleveland, OH, United States.
Front Med (Lausanne). 2022 Aug 8;9:938940. doi: 10.3389/fmed.2022.938940. eCollection 2022.
Hypotension is common in propofol anesthesia. Whether remimazolam could reduce intraoperative hypotension remains unknown. We therefore tested the primary hypothesis that remimazolam reduces the incidence of intraoperative hypotension compared with propofol in adult patients undergoing endoscopic submucosal dissection (ESD) surgery.
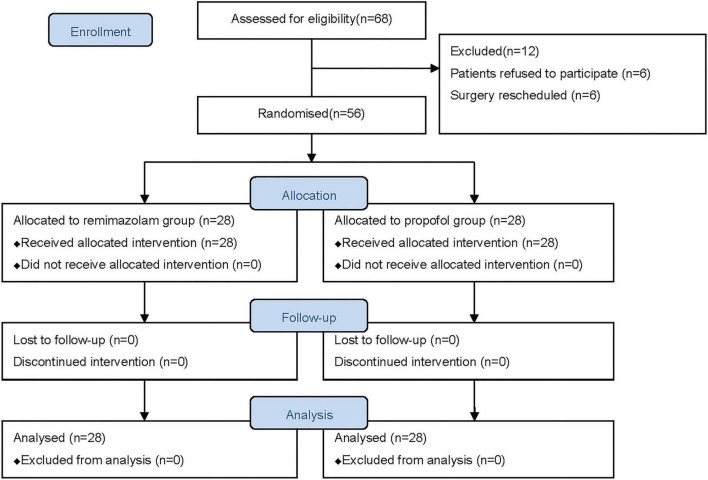
We conducted a prospective trial to compare patients who received either remimazolam or propofol bolus induction and thereafter intravenous infusion. The hemodynamic parameters were measured using CNAP Monitor 500 system. Our primary analysis was to compare the incidence of hypotension defined as systolic blood pressure below 90 mmHg between remimazolam and propofol during the whole anesthesia period.
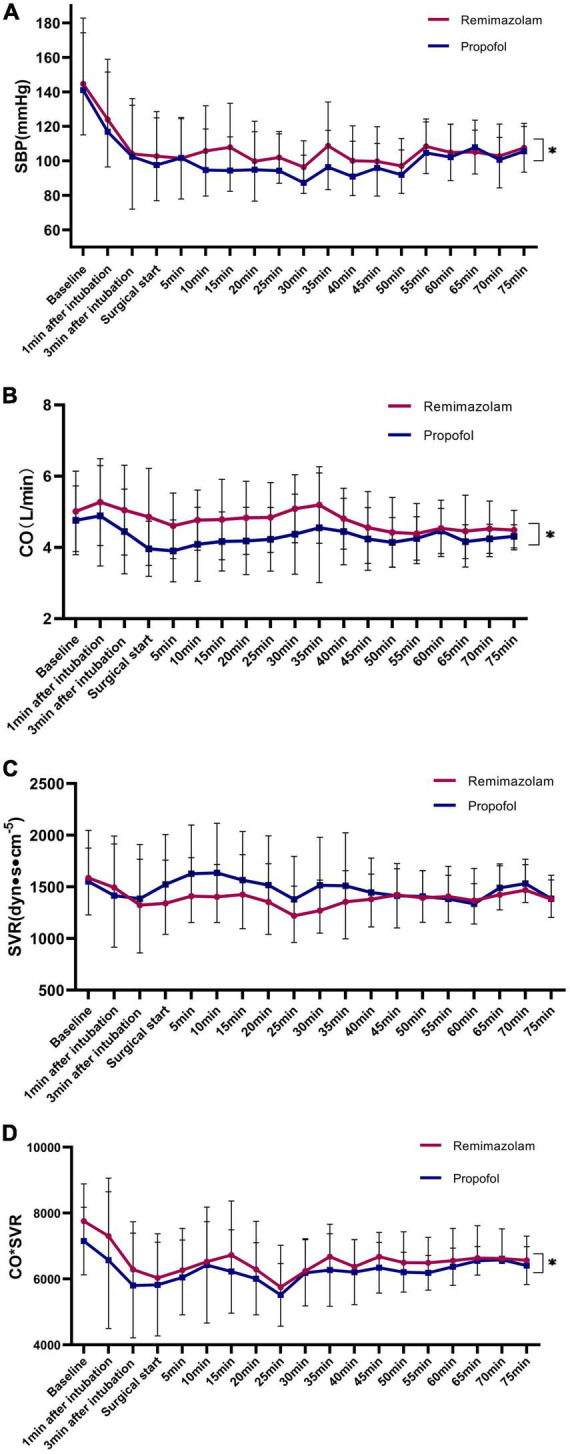
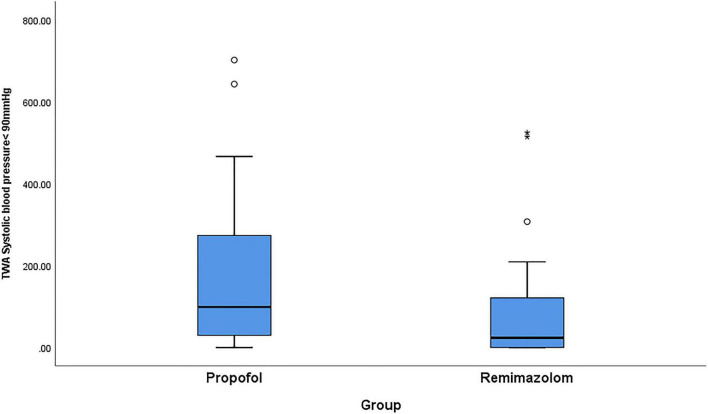
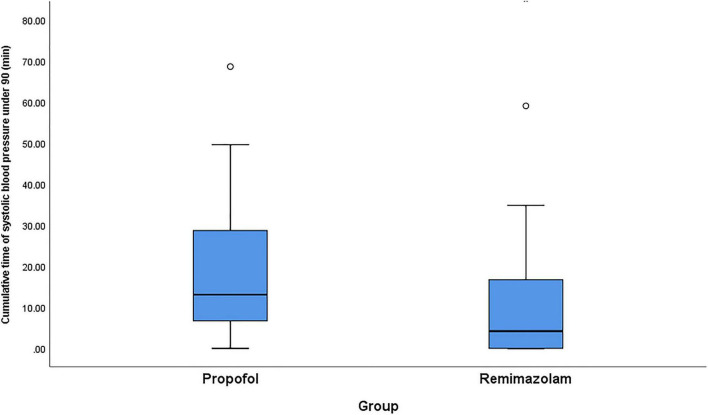
The incidence of hypotension decreased by 50%, from 67.9% in propofol group to 32.1% in remimazolam group ( < 0.01). Patients received less amount of intraoperative phenylephrine in the remimazolam group than the propofol group (0 [0-40] μg vs. 80 [0-200] μg, < 0.01). Time-weighted average and cumulative time of hypotension was lower in remimazolam group compared with propofol group ( < 0.05). Cardiac output continuously measured by CNAP was preserved much better in remimazolam group compared with propofol group ( = 0.01), while systemic vascular resistance did not differ between the groups. The median time from discontinuation until full alertness was 4 [3-11.8] min in the remimazolam group compared with 15 [12.0-19.8] min in the propofol group ( < 0.01).
Remimazolam has better hemodynamic stability than propofol in adult patients undergoing ESD surgery. The benefits of remimazolam on hemodynamic stability and hypotension prevention may be partly contributed to its better preservation of cardiac output.
[http://www.chictr.org.cn/com/25/showproj.aspx?proj=61104], identifier [ChiCTR2000037975].
低血压在丙泊酚麻醉中很常见。瑞马唑仑是否能降低术中低血压尚不清楚。因此,我们检验了主要假设:在接受内镜黏膜下剥离术(ESD)的成年患者中,与丙泊酚相比,瑞马唑仑可降低术中低血压的发生率。
我们进行了一项前瞻性试验,比较接受瑞马唑仑或丙泊酚推注诱导并随后静脉输注的患者。使用CNAP Monitor 500系统测量血流动力学参数。我们的主要分析是比较瑞马唑仑组和丙泊酚组在整个麻醉期间收缩压低于90 mmHg定义的低血压发生率。
低血压发生率降低了50%,从丙泊酚组的67.9%降至瑞马唑仑组的32.1%(P<0.01)。瑞马唑仑组患者术中去氧肾上腺素的用量低于丙泊酚组(0[0 - 40]μg对80[0 - 200]μg,P<0.01)。与丙泊酚组相比,瑞马唑仑组低血压的时间加权平均值和累计时间更低(P<0.05)。与丙泊酚组相比,瑞马唑仑组通过CNAP连续测量的心输出量保持得更好(P = 0.01),而两组之间的全身血管阻力没有差异。瑞马唑仑组从停药到完全清醒的中位时间为4[3 - 11.8]分钟,而丙泊酚组为15[12.0 - 19.8]分钟(P<0.01)。
在接受ESD手术的成年患者中,瑞马唑仑比丙泊酚具有更好的血流动力学稳定性。瑞马唑仑在血流动力学稳定性和预防低血压方面的益处可能部分归因于其对心输出量的更好维持。
[http://www.chictr.org.cn/com/25/showproj.aspx?proj=61104],标识符[ChiCTR2000037975]