Department of Cardiology, Kaiser Permanente West Los Angeles Medical Center, Los Angeles, California.
Department of Clinical Science, Kaiser Permanente Bernard J. Tyson School of Medicine, Pasadena, California.
JAMA Netw Open. 2022 Aug 1;5(8):e2228720. doi: 10.1001/jamanetworkopen.2022.28720.
Prior studies have suggested that participation in home-based cardiac rehabilitation (HBCR) vs center-based cardiac rehabilitation (CBCR) results in similar clinical outcomes in patients with low to moderate risk; however, outcome data from demographically diverse populations and patients who are medically complex are lacking.
To compare hospitalizations, medication adherence, and cardiovascular risk factor control between participants in HBCR vs CBCR.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study was conducted among patients in Kaiser Permanente Southern California (KPSC), an integrated health care system serving approximately 4.7 million patients, who participated in CR between April 1, 2018, and April 30, 2019, and with follow-up through April 30, 2020. Data were analyzed from January 2021 to January 2022.
Participation in 1 or more HBCR or CBCR sessions.
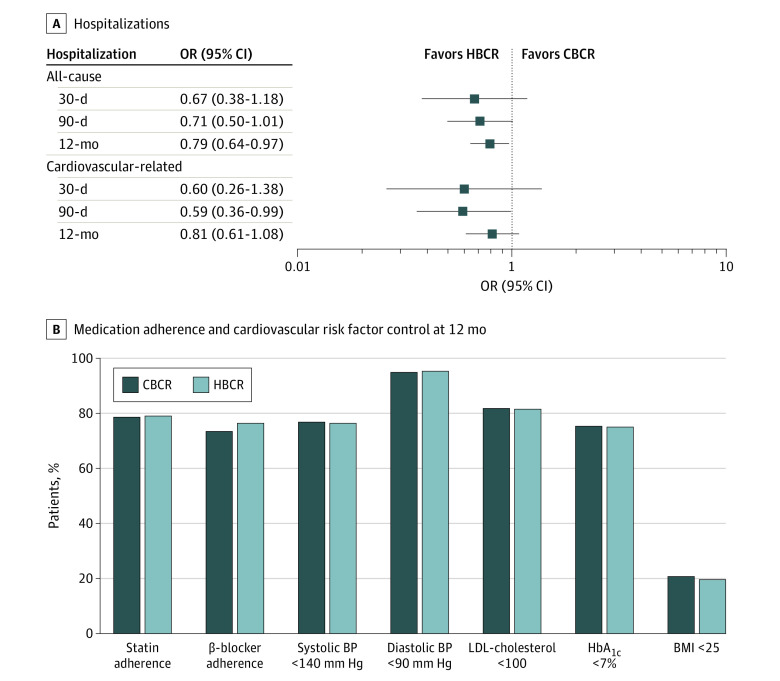
The primary outcome was 12-month all-cause hospitalization. Secondary outcomes included all-cause hospitalizations at 30 and 90 days; 30-day, 90-day, and 12-month cardiovascular hospitalizations; and medication adherence and cardiovascular risk factor control at 12 months. Logistic regression was used to compare hospitalization, medication adherence, and cardiovascular risk factor control, with inverse probability treatment weighting (IPTW) to adjust for demographic and clinical characteristics.
Of 2556 patients who participated in CR (mean [SD] age, 66.7 [11.2] years; 754 [29.5%] women; 1196 participants [46.8%] with Charlson Comorbidity Index ≥4), there were 289 Asian or Pacific Islander patients (11.3%), 193 Black patients (7.6%), 611 Hispanic patients (23.9%), and 1419 White patients (55.5%). A total of 1241 participants (48.5%) received HBCR and 1315 participants (51.5%) received CBCR. After IPTW, patients who received HBCR had lower odds of hospitalization at 12 months (odds ratio [OR], 0.79; 95% CI, 0.64-0.97) but similar odds of adherence to β-blockers (OR, 1.18; 95% CI, 0.98-1.42) and statins (OR, 1.02; 95% CI, 0.84-1.25) and of control of blood pressure (OR, 0.98; 95% CI, 0.81-1.17), low-density lipoprotein cholesterol (OR, 0.98; 95% CI, 0.81-1.20), and hemoglobin A1c (OR, 0.98; 95% CI, 0.82-1.18) at 12 months compared with patients who received CBCR.
These findings suggest that HBCR in a demographically diverse population, including patients with high risk who are medically complex, was associated with fewer hospitalizations at 12 months compared with patients who participated in CBCR. This study strengthens the evidence supporting HBCR in previously understudied patient populations.
先前的研究表明,在低危到中危患者中,家庭为基础的心脏康复(HBCR)与中心为基础的心脏康复(CBCR)相比,其临床结果相似;然而,缺乏来自人口统计学上多样化的人群和医疗复杂的患者的数据。
比较 HBCR 与 CBCR 参与者的住院情况、药物依从性和心血管风险因素控制情况。
设计、地点和参与者:这是一项回顾性队列研究,在 Kaiser Permanente Southern California(KPSC)的患者中进行,该医疗系统为大约 470 万患者提供服务,他们在 2018 年 4 月 1 日至 2019 年 4 月 30 日期间参加了 CR,并在 2020 年 4 月 30 日之前进行了随访。数据分析于 2021 年 1 月至 2022 年 1 月进行。
参加 1 次或多次 HBCR 或 CBCR 课程。
主要结果是 12 个月的全因住院治疗。次要结果包括 30 天和 90 天的全因住院治疗;30 天、90 天和 12 个月的心血管住院治疗;以及 12 个月的药物依从性和心血管风险因素控制。使用逻辑回归比较住院治疗、药物依从性和心血管风险因素控制情况,并使用逆概率治疗加权(IPTW)调整人口统计学和临床特征。
在 2556 名参加 CR 的患者中(平均[SD]年龄,66.7[11.2]岁;754[29.5%]名女性;Charlson 合并症指数≥4 的 1196 名患者[46.8%]),有 289 名亚裔或太平洋岛民患者(11.3%),193 名黑人患者(7.6%),611 名西班牙裔患者(23.9%)和 1419 名白人患者(55.5%)。共有 1241 名患者(48.5%)接受 HBCR,1315 名患者(51.5%)接受 CBCR。在进行 IPTW 后,接受 HBCR 的患者在 12 个月时的住院率较低(比值比[OR],0.79;95%置信区间[CI],0.64-0.97),但在接受β受体阻滞剂(OR,1.18;95%CI,0.98-1.42)和他汀类药物(OR,1.02;95%CI,0.84-1.25)的依从性,以及控制血压(OR,0.98;95%CI,0.81-1.17)、低密度脂蛋白胆固醇(OR,0.98;95%CI,0.81-1.20)和血红蛋白 A1c(OR,0.98;95%CI,0.82-1.18)方面的控制情况与接受 CBCR 的患者相似。
这些发现表明,在人口统计学上多样化的人群中,包括医疗复杂的高危患者,与接受 CBCR 的患者相比,HBCR 与 12 个月时的住院率较低相关。这项研究加强了支持在以前研究不足的患者人群中进行 HBCR 的证据。