MMWR Surveill Summ. 2022 Aug 19;71(7):1-14. doi: 10.15585/mmwr.ss7107a1.
PROBLEM/CONDITION: Coccidioidomycosis, histoplasmosis, and blastomycosis are underdiagnosed fungal diseases that often mimic bacterial or viral pneumonia and can cause disseminated disease and death. These diseases are caused by inhalation of fungal spores that have distinct geographic niches in the environment (e.g., soil or dust), and distribution is highly susceptible to climate changes such as expanding arid regions for coccidioidomycosis, the northward expansion of histoplasmosis, and areas like New York reporting cases of blastomycosis previously thought to be nonendemic. The national incidence of coccidioidomycosis, histoplasmosis, and blastomycosis is poorly characterized.
The National Notifiable Diseases Surveillance System (NNDSS) tracks cases of coccidioidomycosis, a nationally notifiable condition reported to CDC by 26 states and the District of Columbia. Neither histoplasmosis nor blastomycosis is a nationally notifiable condition; however, histoplasmosis is voluntarily reported in 13 states and blastomycosis in five states. Health departments classify cases based on the definitions established by the Council of State and Territorial Epidemiologists.
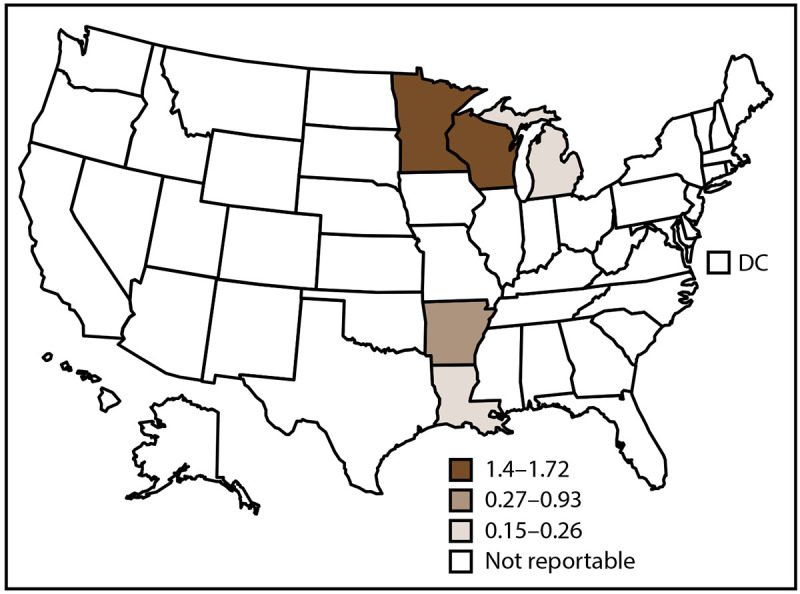
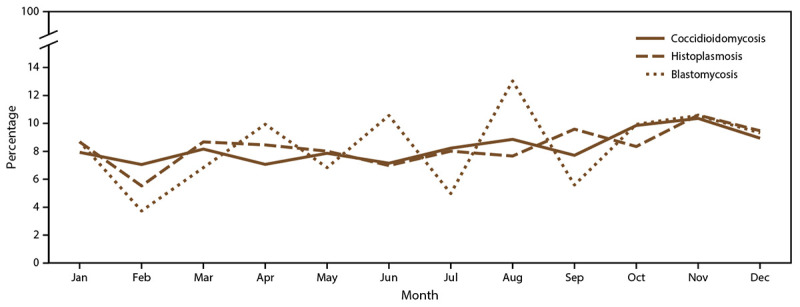
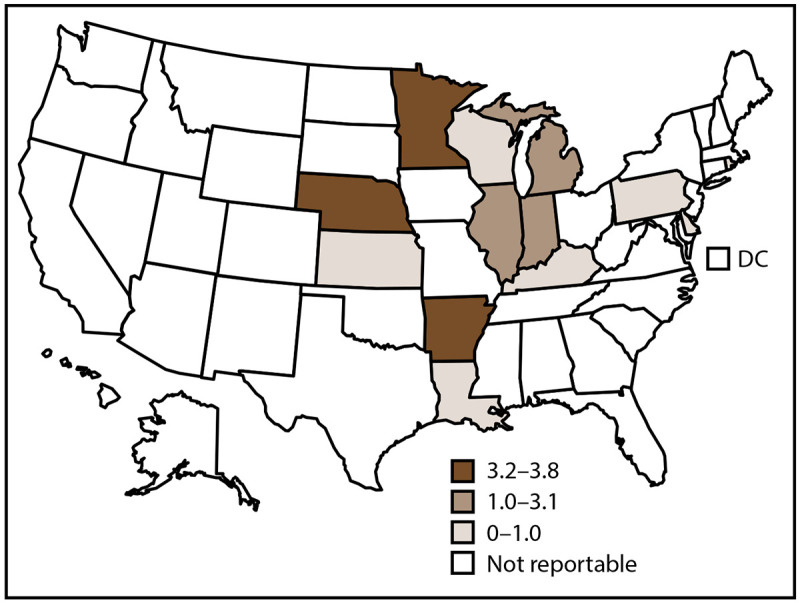
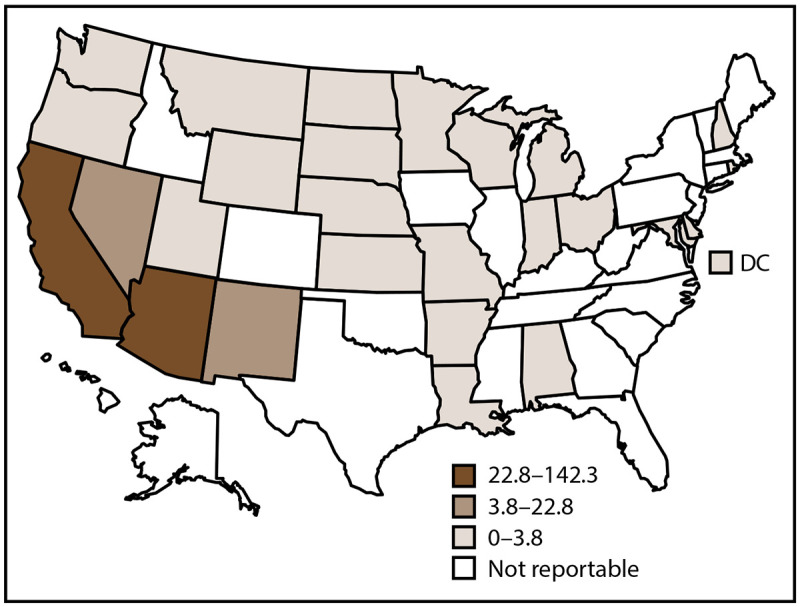
In 2019, a total of 20,061 confirmed coccidioidomycosis, 1,124 confirmed and probable histoplasmosis, and 240 confirmed and probable blastomycosis cases were reported to CDC. Arizona and California reported 97% of coccidioidomycosis cases, and Minnesota and Wisconsin reported 75% of blastomycosis cases. Illinois reported the greatest percentage (26%) of histoplasmosis cases. All three diseases were more common among males, and the proportion for blastomycosis (70%) was substantially higher than for histoplasmosis (56%) or coccidioidomycosis (52%). Coccidioidomycosis incidence was approximately four times higher for non-Hispanic American Indian or Alaska Native (AI/AN) persons (17.3 per 100,000 population) and almost three times higher for Hispanic or Latino persons (11.2) compared with non-Hispanic White (White) persons (4.1). Histoplasmosis incidence was similar across racial and ethnic categories (range: 0.9-1.3). Blastomycosis incidence was approximately six times as high among AI/AN persons (4.5) and approximately twice as high among non-Hispanic Asian and Native Hawaiian or other Pacific Islander persons (1.6) compared with White persons (0.7). More than one half of histoplasmosis (54%) and blastomycosis (65%) patients were hospitalized, and 5% of histoplasmosis and 9% of blastomycosis patients died. States in which coccidioidomycosis is not known to be endemic had more cases in spring (March, April, and May) than during other seasons, whereas the number of cases peaked slightly in autumn (September, October, and November) for histoplasmosis and in winter (December, January, and February) for blastomycosis.
Coccidioidomycosis, histoplasmosis, and blastomycosis are diseases occurring in geographical niches within the United States. These diseases cause substantial illness, with approximately 20,000 coccidioidomycosis cases reported in 2019. Although substantially fewer histoplasmosis and blastomycosis cases were reported, surveillance was much more limited and underdiagnosis was likely, as evidenced by high hospitalization and death rates. This suggests that persons with milder symptoms might not seek medical evaluation and the symptoms self-resolve or the illnesses are misdiagnosed as other, more common respiratory diseases.
Improved surveillance is necessary to better characterize coccidioidomycosis severity and to improve detection of histoplasmosis and blastomycosis. These findings might guide improvements in testing practices that enable timely diagnosis and treatment of fungal diseases. Clinicians and health care professionals should consider coccidioidomycosis, histoplasmosis, and blastomycosis in patients with community-acquired pneumonia or other acute infections of the lower respiratory tract who live in or have traveled to areas where the causative fungi are known to be present in the environment. Culturally appropriate tailored educational messages might help improve diagnosis and treatment. Public health response to these three diseases is hindered because information gathered from states' routine surveillance does not include data on populations at risk and sources of exposure. Broader surveillance that includes expansion to other states, and more detail about potential exposures and relevant host factors can describe epidemiologic trends, populations at risk, and disease prevention strategies.
问题/情况:球孢子菌病、组织胞浆菌病和芽生菌病是被低估的真菌病,常类似于细菌性或病毒性肺炎,可导致播散性疾病和死亡。这些疾病是由吸入具有特定地理小生境(如土壤或灰尘)的真菌孢子引起的,其分布极易受到气候变化的影响,例如球孢子菌病的干旱地区扩大、组织胞浆菌病的向北扩展以及像纽约这样以前被认为是非地方性的芽生菌病的地区。球孢子菌病、组织胞浆菌病和芽生菌病的国家发病率特征描述较差。
2019 年。
国家传染病监测系统(NNDSS)跟踪球孢子菌病的病例,这是一种全国性传染病,由 26 个州和哥伦比亚特区向疾控中心报告。组织胞浆菌病和芽生菌病均非全国性传染病;然而,在 13 个州和 5 个州自愿报告组织胞浆菌病和芽生菌病。卫生部门根据州和地区传染病专家委员会制定的定义对病例进行分类。
2019 年,共报告了 20061 例确诊球孢子菌病、1124 例确诊和可能的组织胞浆菌病以及 240 例确诊和可能的芽生菌病。亚利桑那州和加利福尼亚州报告了 97%的球孢子菌病病例,明尼苏达州和威斯康星州报告了 75%的芽生菌病病例。伊利诺伊州报告的组织胞浆菌病病例占比最大(26%)。这三种疾病在男性中更为常见,芽生菌病(70%)的比例明显高于组织胞浆菌病(56%)或球孢子菌病(52%)。非西班牙裔美国印第安人或阿拉斯加原住民(AI/AN)人群的球孢子菌病发病率约为每 10 万人 17.3 例(4.1),西班牙裔或拉丁裔人群的发病率约为每 10 万人 11.2 例(11.2),而非西班牙裔白人(White)人群的发病率约为每 10 万人 4.1 例。组织胞浆菌病的发病率在不同种族和族裔群体中相似(范围:0.9-1.3)。芽生菌病的发病率在 AI/AN 人群中约为每 10 万人 4.5 例,在非西班牙裔亚洲人和夏威夷原住民或其他太平洋岛民中约为每 10 万人 1.6 例,而在白人中约为每 10 万人 0.7 例。超过一半的组织胞浆菌病(54%)和芽生菌病(65%)患者住院,5%的组织胞浆菌病和 9%的芽生菌病患者死亡。在已知没有球孢子菌病地方性流行的州,春季(3 月、4 月和 5 月)的病例数多于其他季节,而组织胞浆菌病的病例数在秋季(9 月、10 月和 11 月)略有增加,芽生菌病的病例数在冬季(12 月、1 月和 2 月)增加。
球孢子菌病、组织胞浆菌病和芽生菌病是发生在美国地理小生境内的疾病。这些疾病会导致严重的疾病,2019 年报告了约 20000 例球孢子菌病病例。尽管组织胞浆菌病和芽生菌病的报告病例数要少得多,但监测范围要窄得多,而且由于高住院率和死亡率,很可能存在漏诊。这表明,症状较轻的患者可能不会寻求医疗评估,症状自行缓解,或者被误诊为其他更常见的呼吸道疾病。
需要改进监测,以更好地描述球孢子菌病的严重程度,并提高组织胞浆菌病和芽生菌病的检出率。这些发现可能有助于改进检测实践,从而实现真菌病的及时诊断和治疗。临床医生和医疗保健专业人员应考虑在社区获得性肺炎或其他急性下呼吸道感染的患者中,考虑球孢子菌病、组织胞浆菌病和芽生菌病,这些患者居住或曾前往已知存在环境中致病真菌的地区。具有文化适应性的定制教育信息可能有助于改善诊断和治疗。由于各州常规监测收集的信息不包括有关高危人群和接触源的信息,因此这些三种疾病的公共卫生应对受到阻碍。扩大到其他州的更广泛监测以及有关潜在暴露和相关宿主因素的更详细信息,可以描述流行病学趋势、高危人群和疾病预防策略。