Department of Anatomy and Physiology, The University of Melbourne, Parkville 3010, Australia.
Graduate Institute of Clinical Medicine, College of Medicine, National Taiwan University, Taipei 10663, Taiwan.
Biomolecules. 2022 Aug 10;12(8):1101. doi: 10.3390/biom12081101.
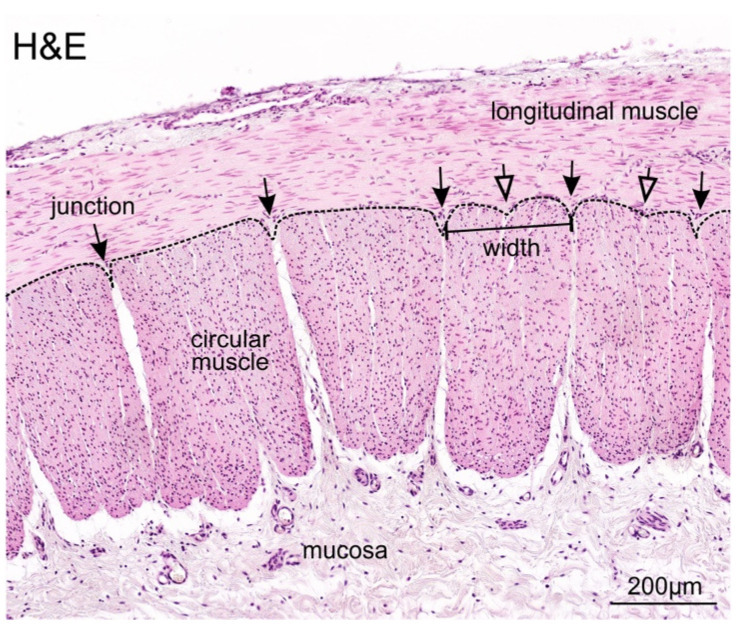
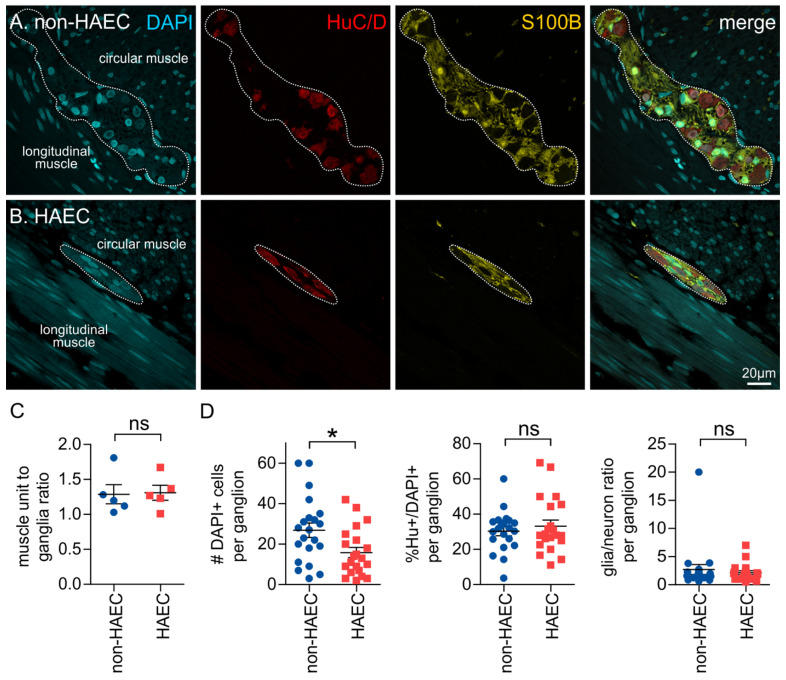
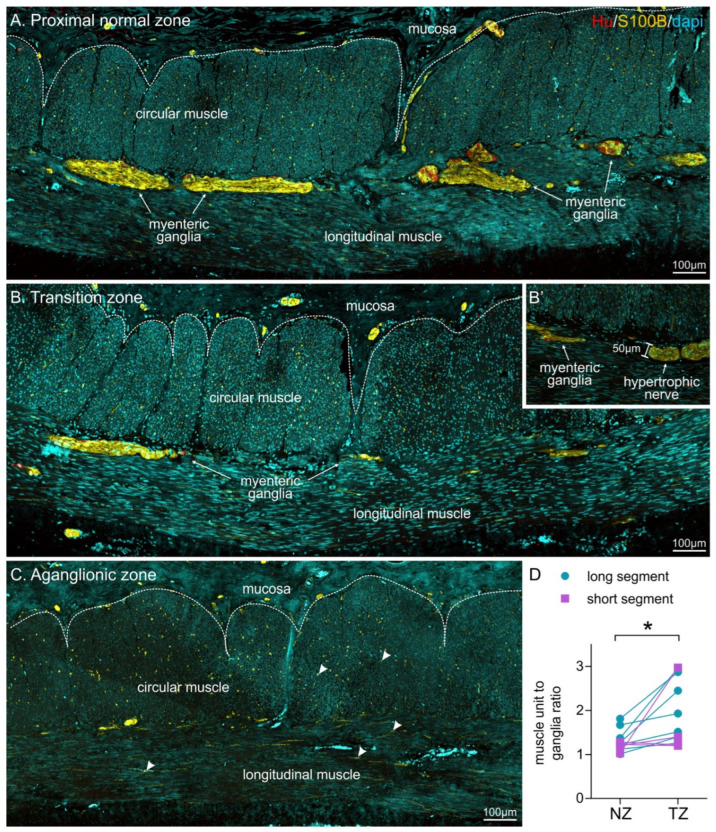
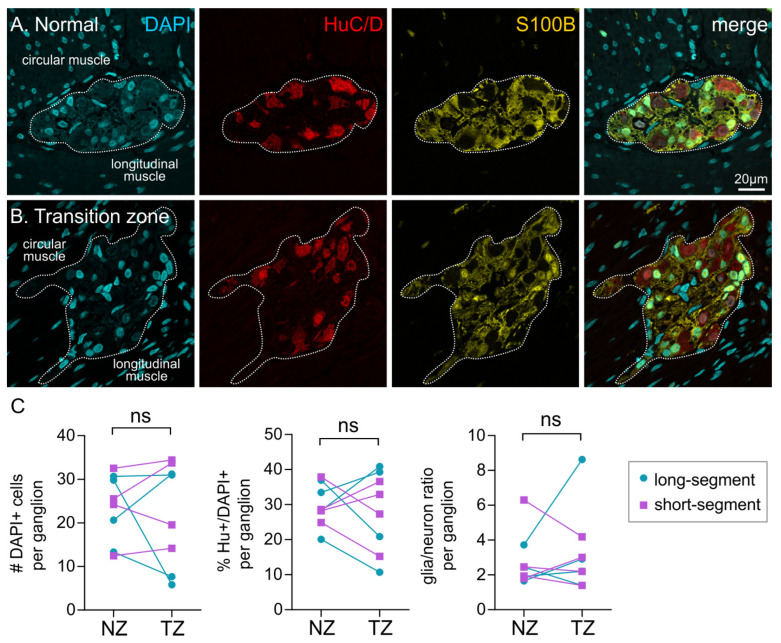
Hirschsprung disease (HSCR) is characterised by the absence of enteric ganglia along variable lengths of the distal bowel. Current gold standard treatment involves the surgical resection of the defective, aganglionic bowel. Clear and reliable distinction of the normoganglionated bowel from the transition zone is key for successful resection of the entire defective bowel, and the avoidance of subsequent postoperative complications. However, the intraoperative nature of the tissue analysis and the variability of patient samples, sample preparation, and operator objectivity, make reproducible identification of the transition zone difficult. Here, we have described a novel method for using muscle units as a distinctive landmark for quantifying the density of enteric ganglia in resection specimens from HSCR patients. We show that the muscle unit to ganglion ratio is greater in the transition zone when compared with the proximal, normoganglionated region for long-segment HSCR patients. Patients with short-segment HSCR were also investigated, however, the muscle unit to ganglion ratio was not significantly different in these patients. Immunohistochemical examination of individual ganglia showed that there were no differences in the proportions of either enteric neurons or glial cells through the different regions of the resected colon. In addition, we identified that the size of enteric ganglia was smaller for patients that went on to develop HSCR associated enterocolitis; although the density of ganglia, as determined by the muscle unit to ganglia ratio, was not different when compared with patients that had no further complications. This suggests that subtle changes in the enteric nervous system, even in the "normoganglionated" colon, could be involved in changes in immune function and subsequent bacterial dysbiosis.
先天性巨结肠(HSCR)的特征是远端肠道的可变长度缺乏肠神经节。目前的金标准治疗方法包括手术切除有缺陷的无神经节肠段。明确和可靠地区分正常神经节肠段和过渡区是成功切除整个缺陷肠段并避免术后并发症的关键。然而,组织分析的术中性质以及患者样本、样本制备和操作者客观性的可变性,使得过渡区的可重复性识别变得困难。在这里,我们描述了一种使用肌节作为标记物来定量分析 HSCR 患者手术切除标本中肠神经节密度的新方法。我们发现,与近端正常神经节肠段相比,长节段 HSCR 患者的过渡区肌节与神经节的比值更大。我们还研究了短节段 HSCR 患者,但这些患者的肌节与神经节的比值没有显著差异。对单个神经节的免疫组织化学检查表明,在不同的结肠切除区域,肠神经元或神经胶质细胞的比例没有差异。此外,我们发现,发生 HSCR 相关结肠炎的患者的肠神经节较小;尽管通过肌节与神经节的比值来确定,与没有进一步并发症的患者相比,神经节的密度没有差异。这表明,即使在“正常神经节”结肠中,肠神经系统的细微变化也可能与免疫功能的改变和随后的细菌失调有关。