Sho Takuya, Suda Goki, Yamamoto Yoshiya, Furuya Ken, Baba Masaru, Ogawa Koji, Kubo Akinori, Tokuchi Yoshimasa, Fu Qingjie, Yang Zijian, Kimura Megumi, Kitagataya Takashi, Maehara Osamu, Ohnishi Shunsuke, Nakamura Akihisa, Yamada Ren, Ohara Masatsugu, Kawagishi Naoki, Natsuizaka Mitsuteru, Nakai Masato, Suzuki Kazuharu, Izumi Takaaki, Meguro Takashi, Terashita Katsumi, Takagi Tomofumi, Ito Jun, Kobayashi Tomoe, Miyagishima Takuto, Sakamoto Naoya
Departments of Gastroenterology and Hepatology, Graduate School of Medicine, Hokkaido University, Sapporo 060-0808, Japan.
Hakodate City Hospital, Hokkaido 041-8680, Japan.
Cancers (Basel). 2022 Aug 15;14(16):3938. doi: 10.3390/cancers14163938.
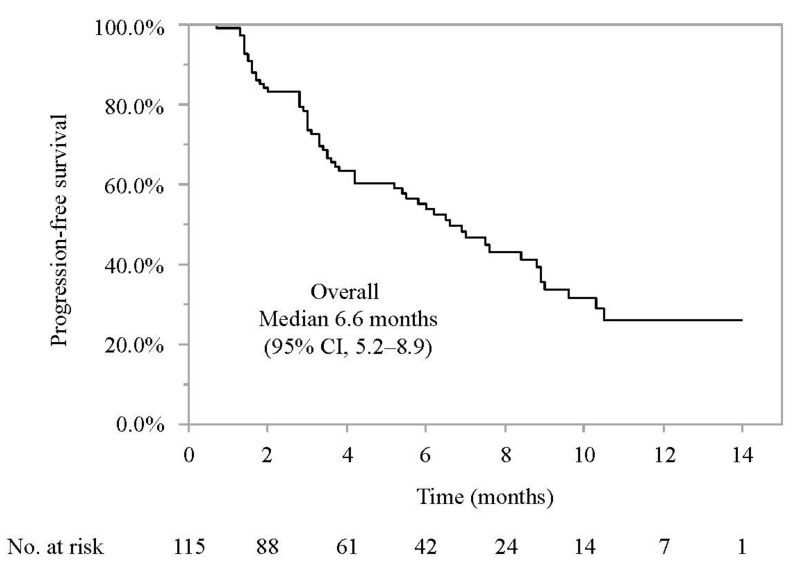
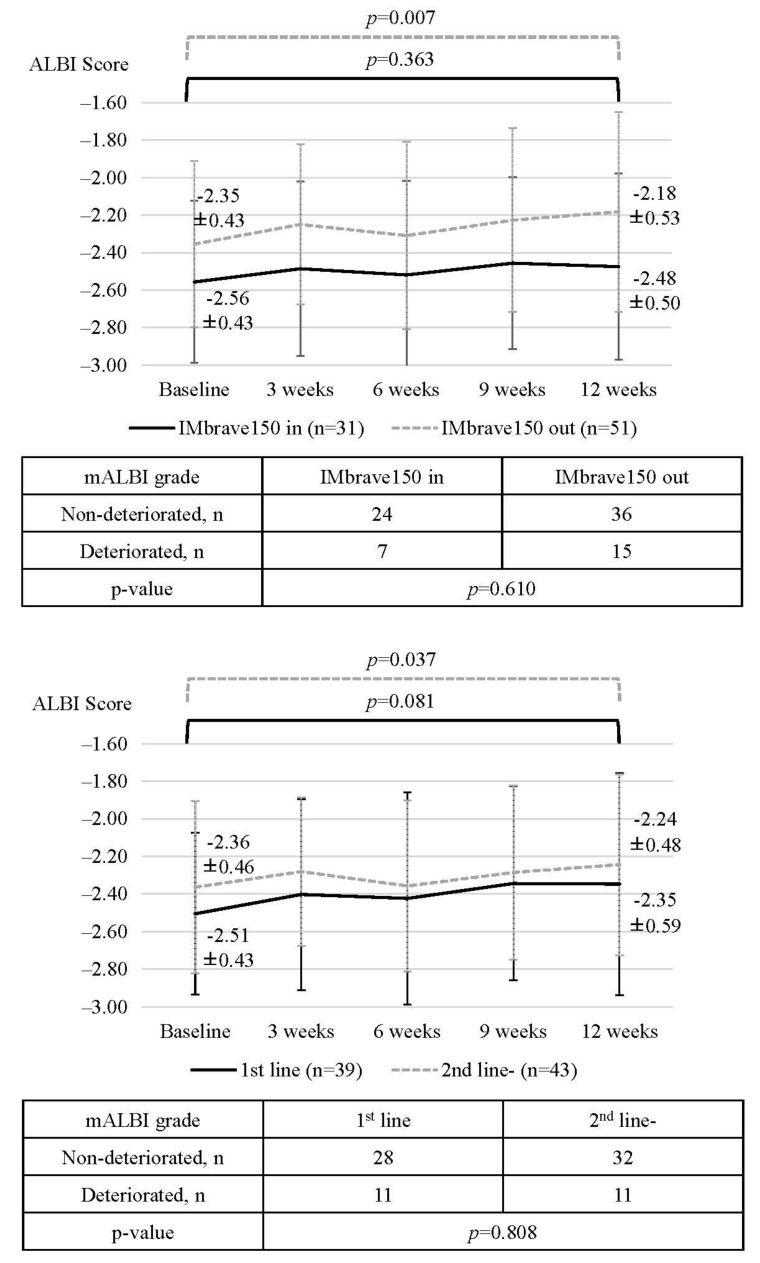
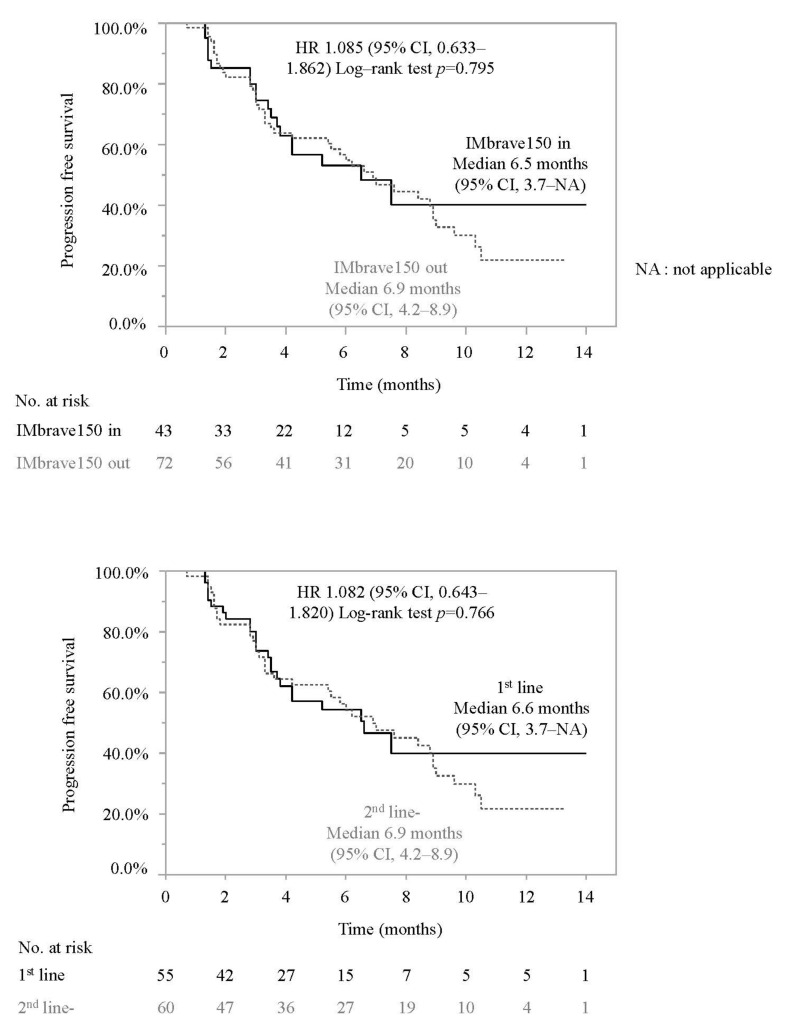
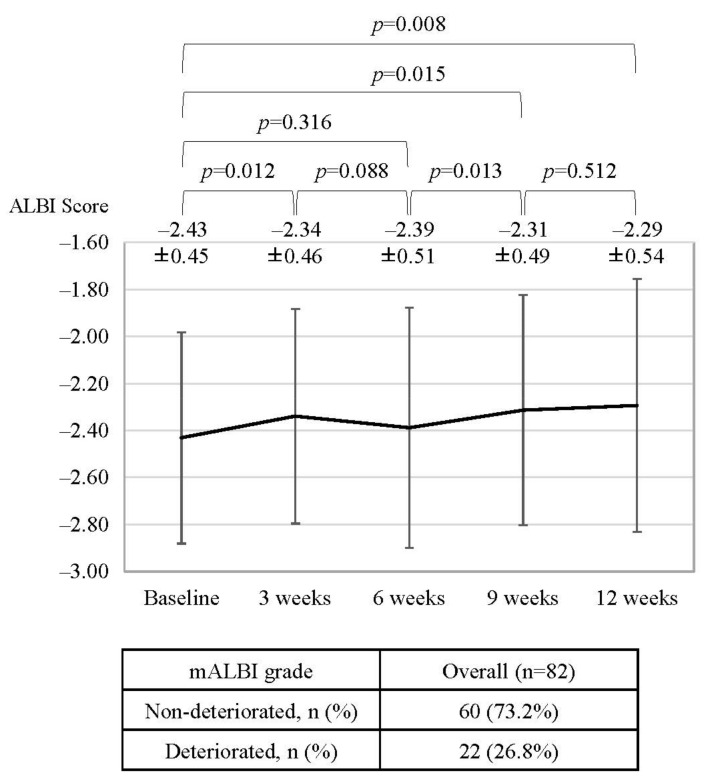
The IMbrave150 trial demonstrated the high efficacy and safety of atezolizumab and bevacizumab for unresectable hepatocellular carcinoma (HCC). In this multicenter study, the efficacy of this combination and its effect on liver functional reserve were evaluated in patients not meeting the eligibility criteria of IMbrave150. Of 115 patients with unresectable HCC treated with atezolizumab and bevacizumab between October 2020 and January 2022, 72 did not meet the eligibility criteria of IMbrave150, most frequently due to a history of systemic therapy (60/72), platelet counts < 75 × 109/L (7/72), Child-Pugh B (9/72), and 2+ proteinuria (8/72). Atezolizumab and bevacizumab therapy was equally effective for patients who did or did not meet the eligibility criteria (PFS, 6.5 vs. 6.9 months, p = 0.765), consistent with subgroup analyses of histories of systemic therapy, platelet counts, Child-Pugh, and proteinuria. Baseline ALBI scores were worse in patients who did not meet the criteria than in those who did and significantly worsened after treatment initiation in patients not meeting the criteria (baseline vs. 12 weeks; 2.35 ± 0.43 vs. −2.18 ± 0.54; p = 0.007). Accordingly, atezolizumab plus bevacizumab was effective for patients not meeting the eligibility criteria of IMbrave150, although careful monitoring for changes in liver functional reserve is needed.
IMbrave150试验证明了阿替利珠单抗和贝伐单抗治疗不可切除肝细胞癌(HCC)具有高效性和安全性。在这项多中心研究中,对不符合IMbrave150纳入标准的患者评估了该联合用药的疗效及其对肝功能储备的影响。在2020年10月至2022年1月期间接受阿替利珠单抗和贝伐单抗治疗的115例不可切除HCC患者中,72例不符合IMbrave150的纳入标准,最常见的原因是有全身治疗史(60/72)、血小板计数<75×10⁹/L(7/72)、Child-Pugh B级(9/72)和2+蛋白尿(8/72)。阿替利珠单抗和贝伐单抗治疗对符合或不符合纳入标准的患者同样有效(无进展生存期,6.5个月对6.9个月,p = 0.765),这与全身治疗史、血小板计数、Child-Pugh分级和蛋白尿的亚组分析结果一致。不符合标准的患者基线ALBI评分比符合标准的患者更差,且在不符合标准的患者开始治疗后显著恶化(基线时对12周时;2.35±0.43对−2.18±0.54;p = 0.007)。因此,阿替利珠单抗加贝伐单抗对不符合IMbrave150纳入标准的患者有效,尽管需要仔细监测肝功能储备的变化。