Department of Epidemiology, Cardiovascular Disease Prevention and Health Promotion, National Institute of Cardiology, 04-628 Warsaw, Poland.
National Institute of Cardiology, 04-628 Warsaw, Poland.
Int J Environ Res Public Health. 2022 Aug 15;19(16):10038. doi: 10.3390/ijerph191610038.
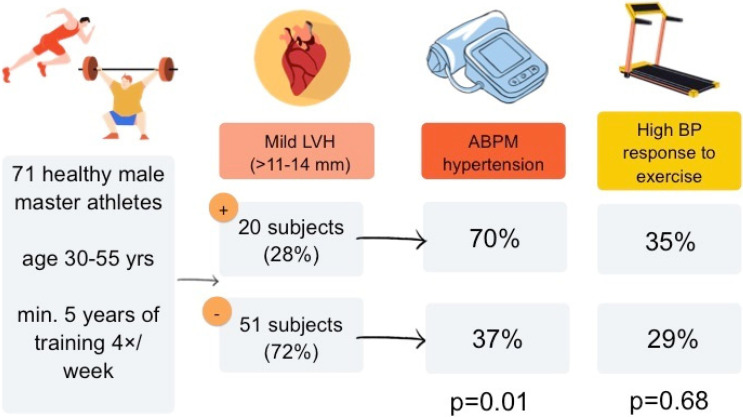
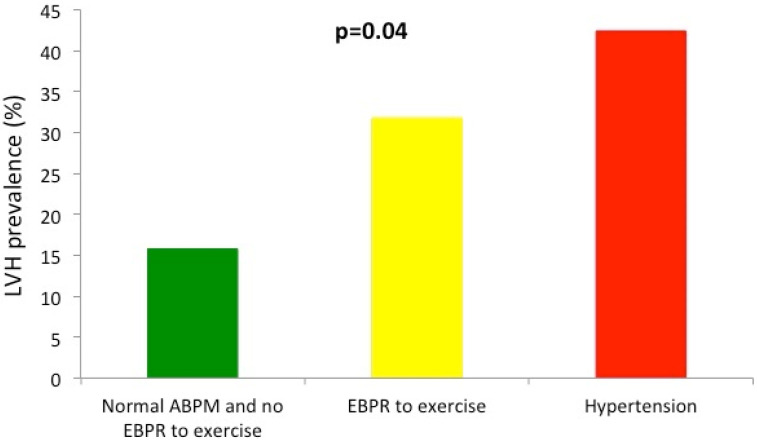
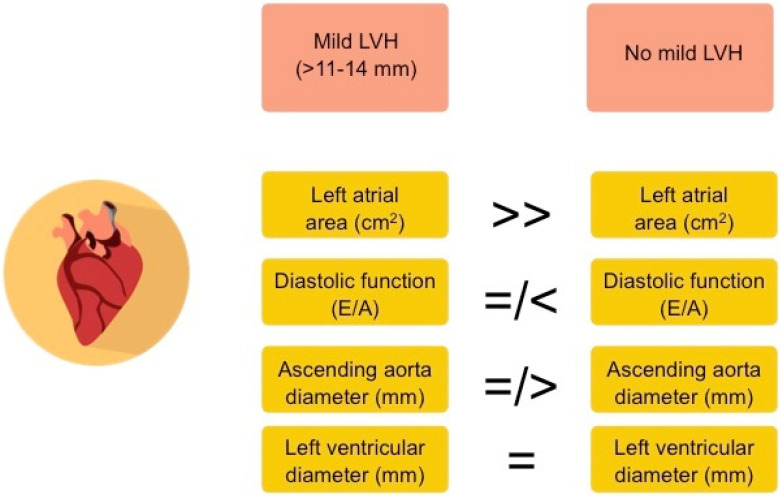
Mild left ventricular hypertrophy (LVH) has been considered as one of the possible structural, physiological adaptations to regular, intensive physical activity. However, it may also appear as one of the subclinical complications of hypertension. In athletes, the differential diagnosis between these two entities may be complicated as regular physical activity may potentially mask the presence of arterial hypertension. We sought to determine the relation between LVH in middle-age athletes and the presence of hypertension. The study included 71 healthy, male long-time amateur athletes (mean age 41 ± 6 years, 83% endurance and 17% power sports) without known hypertension or any other cardiovascular diseases and with normal self-measured and office blood pressure. All subjects underwent resting electrocardiogram, transthoracic echocardiography, maximal exercise test on a treadmill and ambulatory blood pressure monitoring. LVH was diagnosed as left ventricular wall diameter >11 mm. Hypertension was defined as mean 24 h systolic blood pressure (SBP) ≥ 130 mmHg and/or diastolic blood pressure (DBP) ≥ 80 mmHg. Exaggerated blood pressure response (EBPR) to exercise was defined as SBP ≥ 210 mmHg. LVH (range > 11 to 14 mm) was found in 20 subjects (28%) and hypertension was diagnosed in 33 subjects (46%). Athletes with LVH were more likely to have hypertension than those without LVH (70% vs. 37%, p = 0.01). EBPR to exercise was found equally common in athletes with and without LVH (35% vs. 29%, p = 0.68), but more often in subjects with hypertension (51% vs. 13%, p < 0.001). Presence of LVH and hypertension was equally common in the studied endurance and power sport athletes (p = 0.66 and p = 0.79, respectively). In comparison to athletes without LVH, those with LVH had larger left atrial size (26 ± 6 vs. 21 ± 4 cm2, p < 0.001) and a tendency for lower left ventricular diastolic function (E/A 1.2 ± 0.4 vs. 1.5 ± 0.4, p = 0.05) and a larger ascending aorta diameter (34 ± 3 vs. 32 ± 3, p = 0.05), but a similar left ventricular end-diastolic diameter (51 ± 3 vs. 51 ± 4, p = 0.71). The presence of mild left ventricular hypertrophy in middle-age male amateur athletes with normal home and office blood pressure may be considered as a potential sign of masked hypertension. It should not be overlooked as an element of a physiological adaptation to exercise and may warrant further medical evaluation with ambulatory blood pressure monitoring.
轻度左心室肥厚(LVH)被认为是经常进行剧烈运动的一种可能的结构和生理适应。然而,它也可能是高血压的亚临床并发症之一。在运动员中,这两种情况的鉴别诊断可能会变得复杂,因为经常进行体育活动可能会掩盖动脉高血压的存在。我们旨在确定中年运动员的 LVH 与高血压之间的关系。该研究纳入了 71 名健康的男性长期业余运动员(平均年龄 41±6 岁,83%为耐力运动员,17%为力量运动员),他们没有已知的高血压或任何其他心血管疾病,且自我测量和诊室血压正常。所有受试者均接受静息心电图、经胸超声心动图、跑步机最大运动试验和动态血压监测。LVH 诊断为左心室壁直径>11mm。高血压定义为平均 24 小时收缩压(SBP)≥130mmHg 和/或舒张压(DBP)≥80mmHg。运动时血压反应过度(EBPR)定义为 SBP≥210mmHg。20 名受试者(28%)发现 LVH(范围>11 至 14mm),33 名受试者(46%)诊断为高血压。有 LVH 的运动员比没有 LVH 的运动员更容易患高血压(70%比 37%,p=0.01)。有和没有 LVH 的运动员运动时的 EBPR 同样常见(35%比 29%,p=0.68),但在高血压患者中更常见(51%比 13%,p<0.001)。在研究的耐力和力量运动员中,LVH 和高血压的发生率相同(p=0.66 和 p=0.79)。与没有 LVH 的运动员相比,有 LVH 的运动员左心房更大(26±6 比 21±4cm2,p<0.001),左心室舒张功能呈下降趋势(E/A 1.2±0.4 比 1.5±0.4,p=0.05),升主动脉直径更大(34±3 比 32±3,p=0.05),但左心室舒张末期直径相似(51±3 比 51±4,p=0.71)。在家庭和诊室血压正常的中年男性业余运动员中发现轻度左心室肥厚,可能被认为是隐匿性高血压的潜在迹象。不应将其视为运动生理适应的一个因素而忽视,可能需要进行动态血压监测以进一步评估。