Calvino Miryam, Sánchez-Cuadrado Isabel, Gavilán Javier, Lassaletta Luis
Department of Otolaryngology, Hospital Universitario La Paz, IdiPAZ Research Institute, Madrid, Spain.
Biomedical Research Networking Centre on Rare Diseases (CIBERER), Institute of Health Carlos III, Madrid, Spain.
Front Psychol. 2022 Aug 16;13:837366. doi: 10.3389/fpsyg.2022.837366. eCollection 2022.
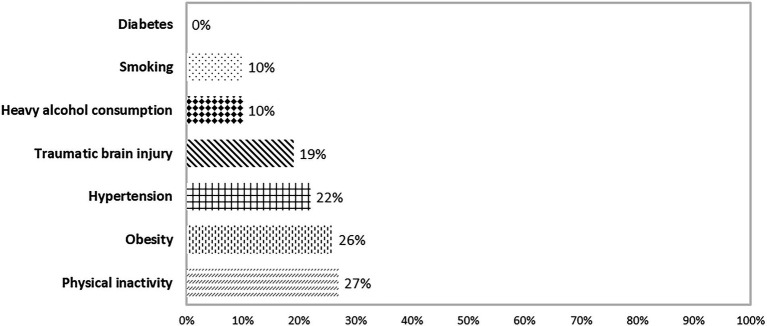
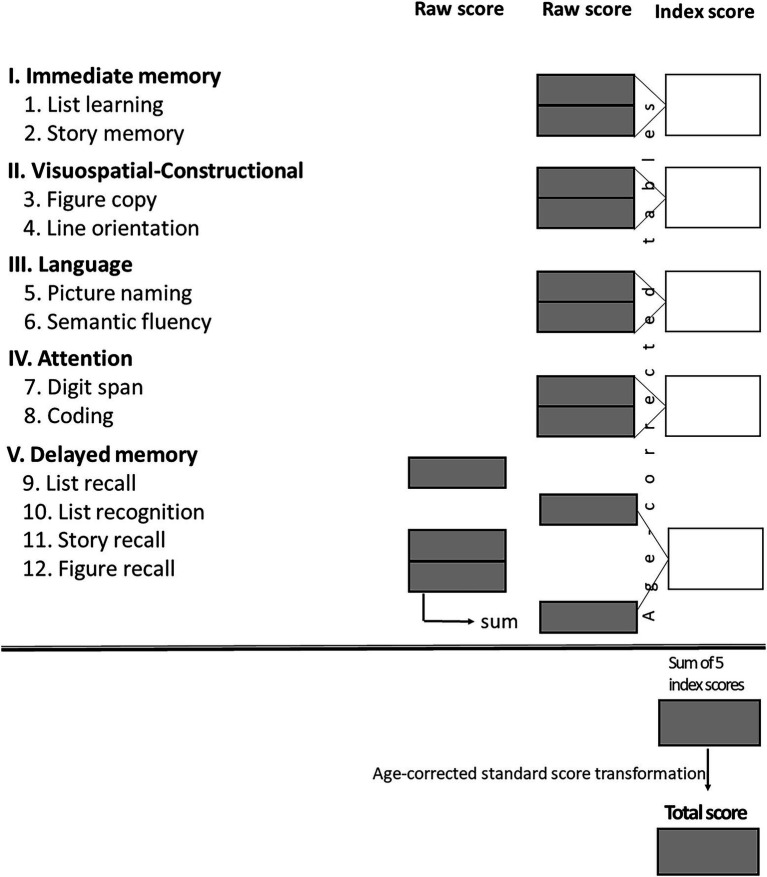
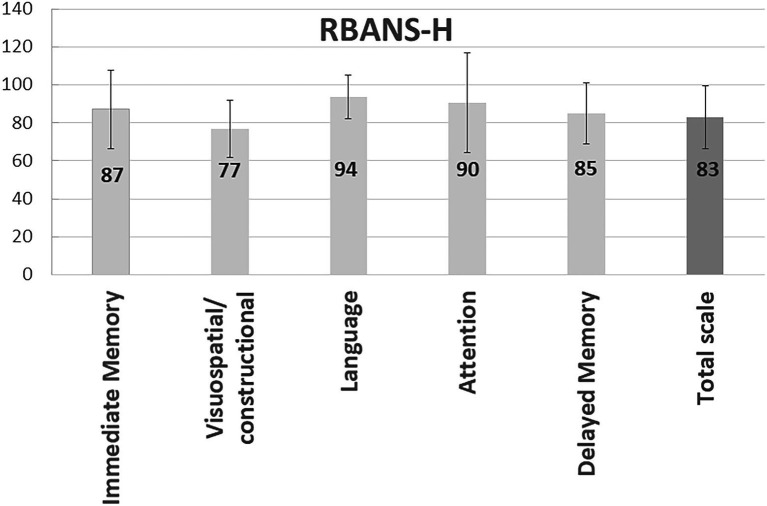
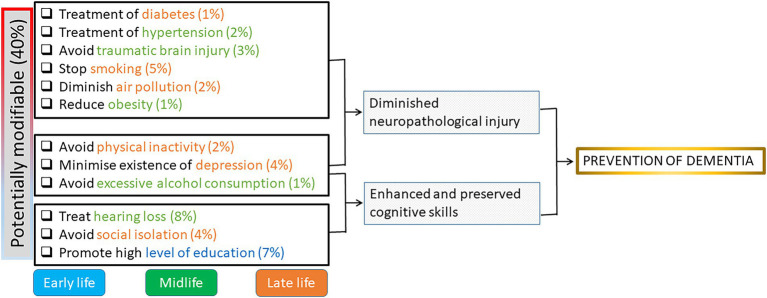
Hearing loss has been identified as a major modifiable risk factors for dementia. Adult candidates for cochlear implantation (CI) represent a population at risk of hearing loss-associated cognitive decline. This study investigated the effect of demographics, habits, and medical and psychological risk factors on cognition within such a cohort. Data from 34 consecutive adults with post-lingual deafness scheduled for CI were analyzed. Pure tone audiometry (PTA4) and Speech Discrimination Score (SDS) were recorded. The Repeatable Battery for Assessment of Neuropsychological Status for Hearing impaired individuals (RBANS-H) was used to measure cognition. Demographics (sex, age, years of education), habits (smoking, alcohol intake, physical inactivity), and medical factors (hypertension, diabetes, traumatic brain injury) were evaluated. Depression was measured using the Hospital Anxiety and Depression Scale (HADS), and social inhibition with the Type D questionnaire (DS14). All participants (mean age 62 ± 15 years) suffered from severe to profound hearing loss (PTA4:129 ± 60 dB; SDS:14 ± 24%). The mean RBANS-H total score was 83 ± 16. Participants reported a mean of years of formal education of 12 ± 5 years. The prevalence of habits and medical risk factors was: physical inactivity (29%), body mass index >30 (28%), traumatic brain injury (25%), hypertension (24%), heavy alcohol consumption (13%), smoking (13%), and diabetes (0%). Regarding psychological factors, the mean scores of social inhibition and depression were 10 ± 6 and 6 ± 5, respectively. The number of years of education was significantly correlated with the RBANS-H total score ( < 0.001), and with the domains "Immediate memory" ( = 0.003), "Visuospatial/constructional" ( < 0.001), and "Attention" ( < 0.001). The mean RBANS-H total score in participants who had university studies or higher level (12/34) was 97 ± 9, with the remaining participants reporting a mean score of 75 ± 15. Men performed better in the "Visuospatial/constructional" ( = 0.008). Physical inactivity was associated with lower scores in the "Delayed memory" ( = 0.031); hypertension correlated with lower RBANS-H total scores ( = 0.025) and "Attention" ( = 0.006). Depression and social inhibition were negatively correlated with RBANS-H total score and with the "Immediate memory," "Visuospatial/constructional," and "Attention" (all < 0.05). In adults with late-onset deafness scheduled to CI, educational level has a significant effect. Additionally, sex, physical inactivity, hypertension, and psychological traits of social inhibition and depression may also influence cognitive status. Long-term studies with more participants would enable us better understand the effects different risk factors on cognitive status.
听力损失已被确认为痴呆症的一个主要可改变风险因素。成年人工耳蜗植入(CI)候选者是面临听力损失相关认知衰退风险的人群。本研究调查了人口统计学因素、习惯以及医学和心理风险因素对该队列人群认知的影响。对34例连续的成年语后聋患者进行CI手术的数据进行了分析。记录了纯音听力测定(PTA4)和言语辨别得分(SDS)。使用针对听力受损个体的可重复神经心理状态评估量表(RBANS-H)来测量认知。评估了人口统计学因素(性别、年龄、受教育年限)、习惯(吸烟、饮酒、缺乏身体活动)和医学因素(高血压、糖尿病、创伤性脑损伤)。使用医院焦虑抑郁量表(HADS)测量抑郁,使用D型问卷(DS14)测量社交抑制。所有参与者(平均年龄62±15岁)患有重度至极重度听力损失(PTA4:129±60dB;SDS:14±24%)。RBANS-H总分平均为83±16。参与者报告的平均正规教育年限为12±5年。习惯和医学风险因素的患病率分别为:缺乏身体活动(29%)、体重指数>30(28%)、创伤性脑损伤(25%)、高血压(24%)、大量饮酒(13%)、吸烟(13%)和糖尿病(0%)。关于心理因素,社交抑制和抑郁的平均得分分别为10±6和6±5。受教育年限与RBANS-H总分显著相关(<0.001),与“即刻记忆”领域(=0.003)、“视觉空间/构建”领域(<0.001)和“注意力”领域(<0.001)也显著相关。接受过大学及以上教育的参与者(12/34)的RBANS-H总分平均为97±9,其余参与者的平均得分为75±15。男性在“视觉空间/构建”领域表现更好(=0.008)。缺乏身体活动与“延迟记忆”得分较低相关(=0.031);高血压与较低的RBANS-H总分(=0.025)和“注意力”得分(=0.006)相关。抑郁和社交抑制与RBANS-H总分以及“即刻记忆”、“视觉空间/构建”和“注意力”均呈负相关(均<0.05)。在计划接受CI的迟发性聋成年患者中,教育水平有显著影响。此外,性别、缺乏身体活动、高血压以及社交抑制和抑郁等心理特征也可能影响认知状态。更多参与者的长期研究将使我们能够更好地了解不同风险因素对认知状态的影响。