ISGlobal, Hospital Clínic-Universitat de Barcelona, Barcelona, Spain.
Consorcio de Investigación Biomédica en Red de Epidemiología y Salud Pública (CIBERESP), Madrid, Spain.
PLoS Med. 2022 Sep 2;19(9):e1004084. doi: 10.1371/journal.pmed.1004084. eCollection 2022 Sep.
Malaria is among the top causes of death in adolescent girls (10 to 19 years) globally. Adolescent motherhood is associated with increased risk of adverse maternal and neonatal outcomes. The interaction of malaria, adolescence, and pregnancy is especially relevant in malaria endemic areas, where rates of adolescent pregnancy are high. However, data on burden of malaria among adolescent girls are limited. This study aimed at investigating whether adolescent girls were at a greater risk of experiencing malaria-related outcomes in pregnancy-parasitaemia and clinical disease-than adult women.
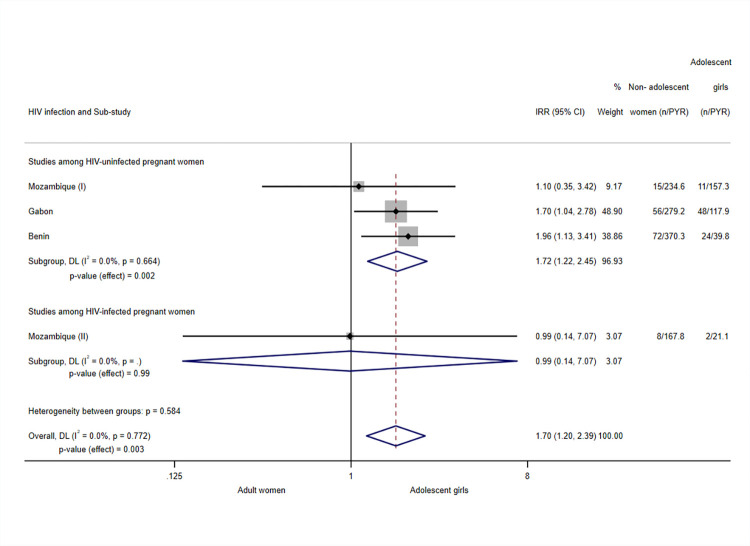
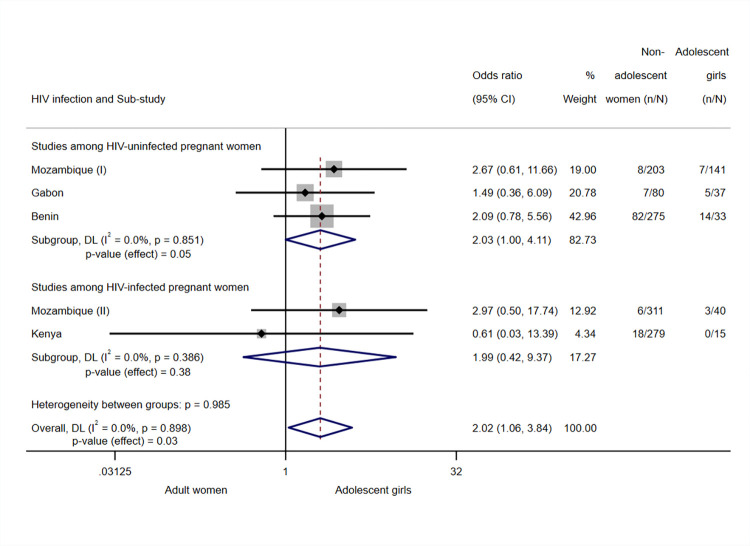
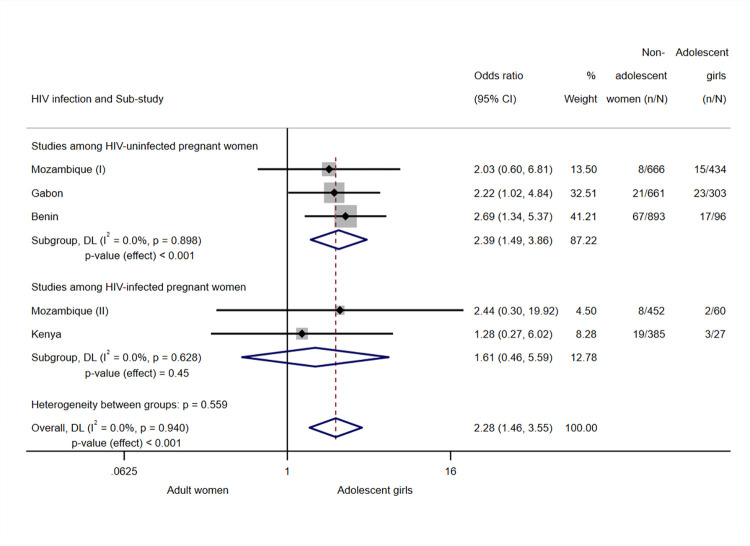
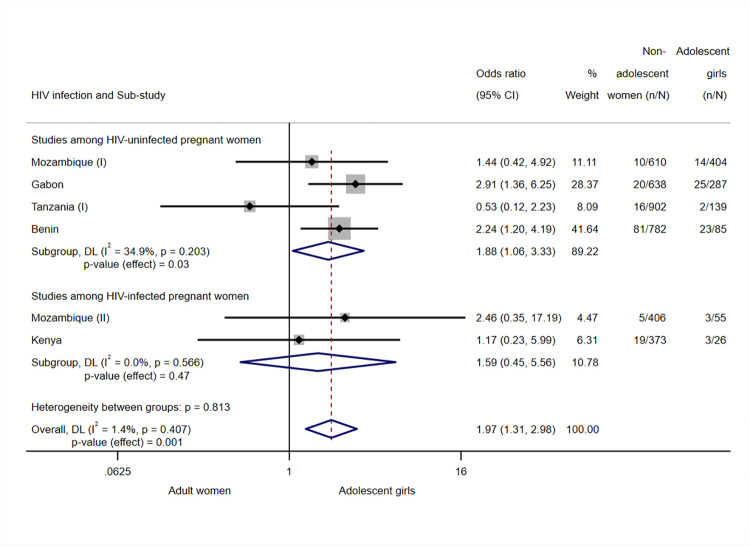
An individual secondary participant-level meta-analysis was conducted using data from 5,804 pregnant women participating in 2 malaria prevention clinical trials in Benin, Gabon, Kenya, Mozambique, and Tanzania between 2009 and 2014. Of the sample, 1,201 participants were adolescent girls with a mean age of 17.5 years (standard deviation (SD) 1.3) and 886 (73.8%) of them primigravidae. Among the 4,603 adult women with mean age of 27.0 years (SD 5.4), 595 (12.9%) were primigravidae. Mean gestational age at enrolment was 20.2 weeks (SD 5.2) and 1,069 (18.4%) participants were HIV-infected. Women were followed monthly until the postpartum visit (1 month to 6 weeks after delivery). This study considered outcomes including clinical episodes during pregnancy, peripheral parasitaemia at delivery, and placental malaria. A 2-stage meta-analysis approach was followed by pooling single multivariable regression results into standard DerSimonian-Laird random-effects models. Adolescent girls were more likely than adult women to present with clinical malaria during pregnancy (incidence risk ratio (IRR) 1.70, 95% confidence interval (CI) 1.20; 2.39, p-value = 0.003, I2 = 0.0%, N = 4,092), peripheral parasitaemia at delivery (odds ratio (OR) 2.28, 95% CI 1.46; 3.55, p-value < 0.001, I2 = 0.0%, N = 3,977), and placental infection (OR 1.97, 95% CI 1.31; 2.98, p-value = 0.001, I2 = 1.4%, N = 4,797). Similar associations were observed among the subgroup of HIV-uninfected participants: IRR 1.72 (95% CI 1.22; 2.45, p-value = 0.002, I2 = 0.0%, N = 3,531) for clinical malaria episodes, OR 2.39 (95% CI 1.49; 3.86, p-value < 0.001, I2 = 0.0%, N = 3,053) for peripheral parasitaemia, and OR 1.88 (95% CI 1.06 to 3.33, p-value = 0.03, I2 = 34.9%, N = 3,847) for placental malaria. Among HIV-infected subgroups statistically significant associations were not observed. Similar associations were found in the subgroup analysis by gravidity. The small sample size and outcome prevalence in specific countries limited the inclusion of some countries in the meta-analysis. Furthermore, peripheral parasitaemia and placental malaria presented a considerable level of missing data-12.6% and 18.2% of participants had missing data on those outcomes, respectively. Given the original scope of the clinical trials, asymptomatic malaria infection was only assessed at the end of pregnancy through peripheral and placental parasitaemia.
In this study, we observed that adolescent girls in sub-Saharan Africa (SSA) are more prone to experience clinical malaria episodes during pregnancy and have peripheral malaria and placental infection at delivery than adult women. Moreover, to the best of our knowledge, for the first time this study disaggregates figures and stratifies analyses by HIV infection. Similar associations were found for both HIV-infected and uninfected women, although those for HIV-infected participants were not statistically significant. Our finding suggests that adolescent girls may benefit from targeted malaria prevention strategies even before they become pregnant.
在全球范围内,疟疾是导致青少年女孩(10 至 19 岁)死亡的主要原因之一。青少年母亲生育与增加不良母婴和新生儿结局的风险相关。疟疾、青春期和妊娠的相互作用在疟疾流行地区尤为重要,这些地区青少年怀孕率很高。然而,关于青春期女孩疟疾负担的数据有限。本研究旨在调查在妊娠-寄生虫血症和临床疾病方面,青春期女孩是否比成年女性更容易经历与疟疾相关的结局。
本研究使用了 2009 年至 2014 年间在贝宁、加蓬、肯尼亚、莫桑比克和坦桑尼亚进行的 2 项疟疾预防临床试验中的 5804 名孕妇的个体二次参与者水平荟萃分析数据。在该样本中,1201 名参与者为青春期女孩,平均年龄为 17.5 岁(标准差 1.3),其中 886 名(73.8%)为初产妇。在 4603 名成年女性中,平均年龄为 27.0 岁(标准差 5.4),其中 595 名(12.9%)为初产妇。入组时的平均妊娠周数为 20.2 周(标准差 5.2),1069 名(18.4%)参与者感染了 HIV。妇女每月随访一次,直至产后访视(分娩后 1 个月至 6 周)。本研究考虑了包括妊娠期间临床发作、分娩时外周寄生虫血症和胎盘疟疾在内的结局。采用两阶段荟萃分析方法,将单个多变量回归结果汇总到标准的 DerSimonian-Laird 随机效应模型中。与成年女性相比,青春期女孩更有可能在妊娠期间出现临床疟疾(发病率风险比 1.70,95%置信区间 1.20-2.39,p 值=0.003,I2=0.0%,N=4092)、分娩时外周寄生虫血症(比值比 2.28,95%置信区间 1.46-3.55,p 值<0.001,I2=0.0%,N=3977)和胎盘感染(比值比 1.97,95%置信区间 1.31-2.98,p 值=0.001,I2=1.4%,N=4797)。在未感染 HIV 的亚组中也观察到类似的关联:临床疟疾发作的发病率风险比为 1.72(95%置信区间 1.22-2.45,p 值=0.002,I2=0.0%,N=3531),外周寄生虫血症的比值比为 2.39(95%置信区间 1.49-3.86,p 值<0.001,I2=0.0%,N=3053),胎盘疟疾的比值比为 1.88(95%置信区间 1.06-3.33,p 值=0.03,I2=34.9%,N=3847)。在感染 HIV 的亚组中,未观察到统计学意义上的关联。在按 gravidity 进行的亚组分析中也发现了类似的关联。特定国家的样本量小和结局患病率限制了一些国家纳入荟萃分析。此外,外周寄生虫血症和胎盘疟疾存在相当大的缺失数据-分别有 12.6%和 18.2%的参与者在这些结局上存在缺失数据。鉴于临床试验的原始范围,仅在妊娠结束时通过外周和胎盘寄生虫血症评估无症状疟疾感染。
在这项研究中,我们观察到撒哈拉以南非洲(SSA)的青春期女孩在妊娠期间更容易出现临床疟疾发作,并且在分娩时外周寄生虫血症和胎盘感染的发生率高于成年女性。此外,据我们所知,这是首次根据 HIV 感染情况对数据进行细分和分层分析。对于感染和未感染 HIV 的妇女,均发现了类似的关联,尽管对于感染 HIV 的参与者,这些关联没有统计学意义。我们的研究结果表明,即使在青春期女孩怀孕之前,她们也可能受益于有针对性的疟疾预防策略。