Pavlovich Stephanie S, Bennett William C, Terinte-Balcan George, Hladik Gerald, Jain Koyal
Division of Hospital Medicine, Department of Medicine, University of North Carolina Health, Chapel Hill, USA.
Division of Nephrology and Hypertension, Department of Medicine, University of North Carolina School of Medicine, Chapel Hill, USA.
Cureus. 2022 Aug 1;14(8):e27560. doi: 10.7759/cureus.27560. eCollection 2022 Aug.
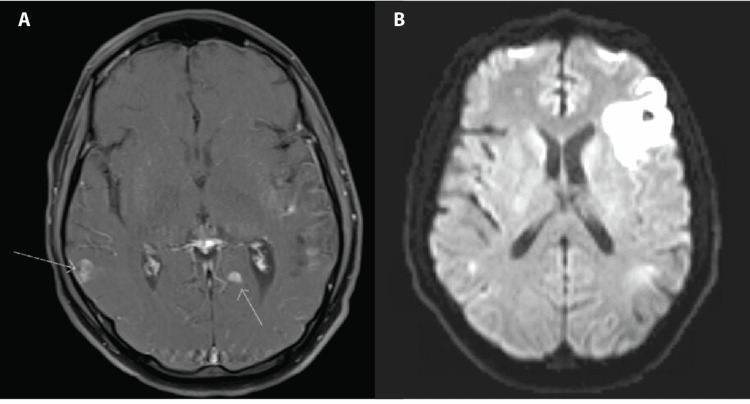
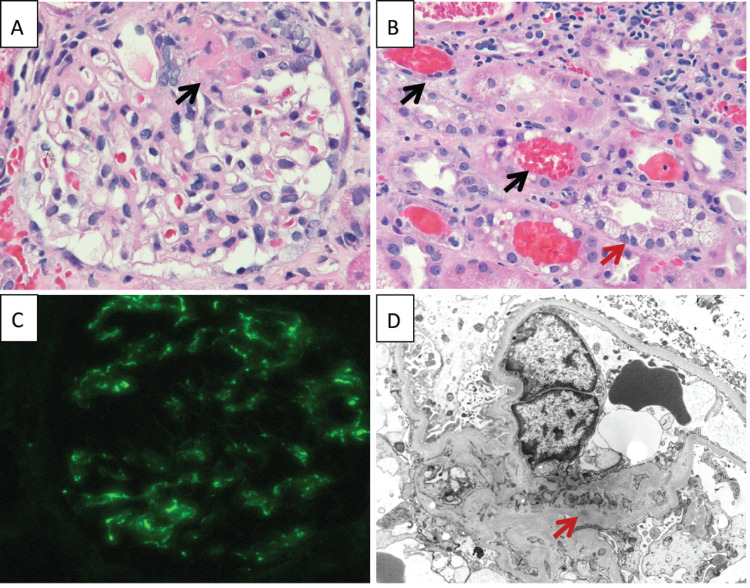
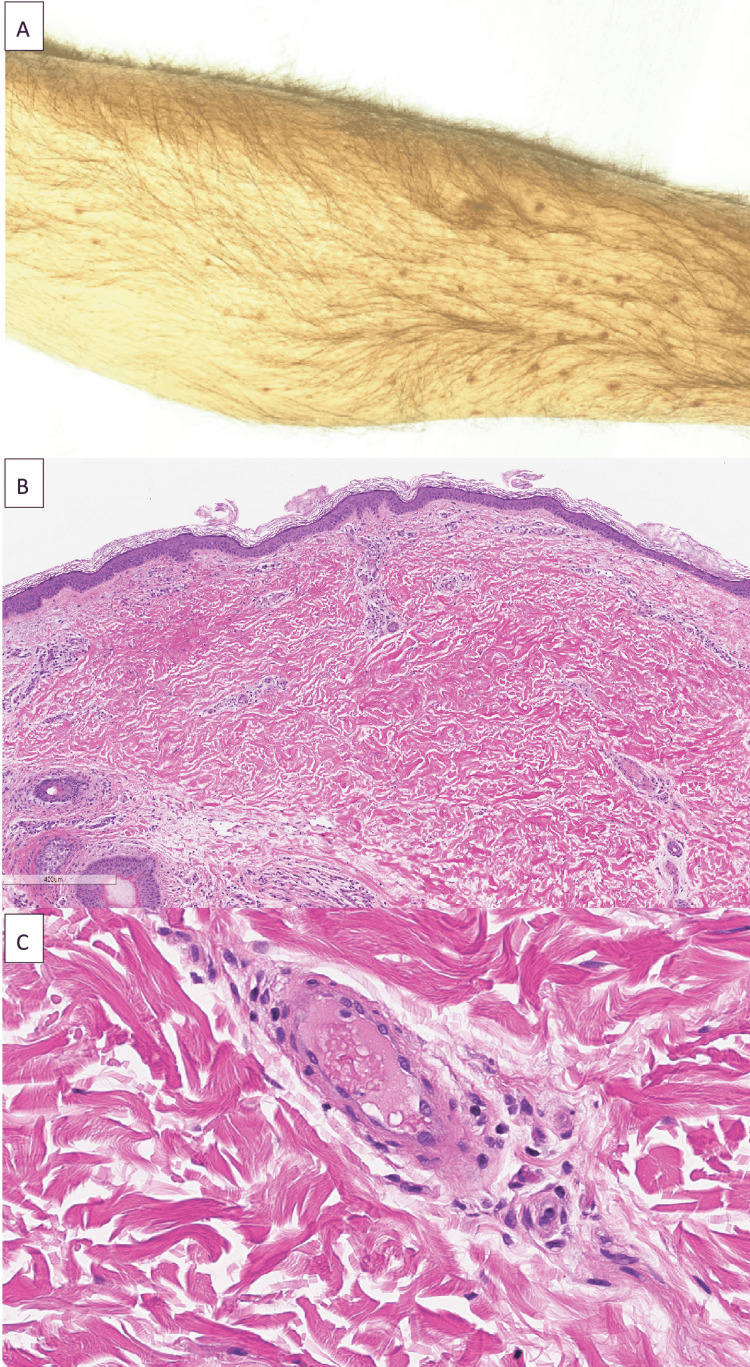
Small-vessel vasculitis has a broad differential with similar clinical presentation and laboratory abnormalities, including petechial rashes, neurologic symptoms, glomerulonephritis, and abnormal inflammatory markers. Biopsy-based diagnosis is critical as the treatment varies by etiology. We report a case of a 41-year-old man with diagnosed cryoglobulinemia and hepatitis C presenting with a petechial rash, altered mental status, and acute kidney injury and ultimately found to have proteinase 3 (PR3)-antineutrophil cytoplasmic antibody (ANCA)-positive vasculitis secondary to infective endocarditis. Skin biopsy was consistent with resolving, but nonspecific vasculitis and MRI showed foci of hemosiderin deposition concerning vasculitic lesions. Blood cultures grew , and he was treated with IV antibiotics. Kidney biopsy showed pauci-immune necrotizing focal segmental glomerulonephritis (GN) and diffuse acute tubular necrosis (ATN). After blood cultures cleared, he was initially treated with mycophenolate for worsening renal function. When the patient stopped antibiotics unexpectedly, his kidney function worsened and improved only after immunosuppression was stopped and antibiotics were restarted. This case highlights the importance of renal biopsy in patients with multiple potential etiologies of GN. The case resolution also reinforces that patients with infective endocarditis causing ANCA-associated GN should be treated with antibiotics in addition to, and possibly instead of, immunosuppression.
小血管炎的鉴别诊断范围广泛,其临床表现和实验室检查异常相似,包括瘀点皮疹、神经系统症状、肾小球肾炎及炎症标志物异常。基于活检的诊断至关重要,因为治疗方案会因病因不同而有所差异。我们报告一例41岁男性病例,该患者诊断为冷球蛋白血症和丙型肝炎,出现瘀点皮疹、精神状态改变及急性肾损伤,最终发现继发于感染性心内膜炎的蛋白酶3(PR3)-抗中性粒细胞胞浆抗体(ANCA)阳性血管炎。皮肤活检结果符合正在消退但非特异性的血管炎表现,磁共振成像(MRI)显示有含铁血黄素沉积灶,提示血管炎性病变。血培养有细菌生长,患者接受了静脉抗生素治疗。肾活检显示寡免疫坏死性局灶节段性肾小球肾炎(GN)和弥漫性急性肾小管坏死(ATN)。血培养转阴后,患者最初因肾功能恶化接受霉酚酸酯治疗。患者意外停用抗生素后,肾功能恶化,仅在停用免疫抑制剂并重新使用抗生素后才有所改善。该病例突出了肾活检在有多种GN潜在病因患者中的重要性。病例的解决也强化了这样一个观点,即对于感染性心内膜炎导致ANCA相关性GN的患者,除免疫抑制治疗外,可能还应使用抗生素治疗,甚至抗生素治疗可替代免疫抑制治疗。