Zhou Ke, Cao Jie, Lin Huahang, Liang Linchuan, Shen Zhongzhong, Wang Lei, Peng Zhiyu, Mei Jiandong
Department of Thoracic Surgery, West China Hospital, Sichuan University, Chengdu, China.
Western China Collaborative Innovation Center for Early Diagnosis and Multidisciplinary Therapy of Lung Cancer, Sichuan University, Chengdu, China.
Front Oncol. 2022 Aug 22;12:962173. doi: 10.3389/fonc.2022.962173. eCollection 2022.
It remains controversial whether the platelet to lymphocyte ratio (PLR) serves as a potential indicator for the efficacy of immunotherapy in advanced lung cancer. This meta-analysis aimed to address this concern.
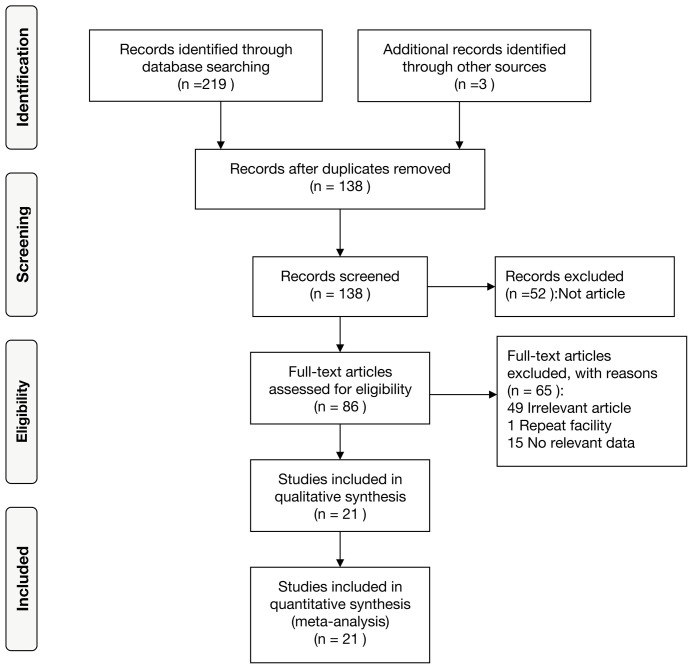
Up to March 2022, we searched PubMed, Embase, Web of Science and the Cochrane Library to retrieve potentially eligible articles. Combined hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated to assess the relationship between PLR and progression-free survival (PFS) as well as overall survival (OS), while the combined odds ratios (ORs) and 95% CIs were estimated to evaluate the relationship between PLR and the objective response rate (ORR) as well as the disease control rate (DCR). Subgroup analyses were further performed to detect the source of heterogeneity and potential predictive value of PLR in different groups in terms of OS and PFS.
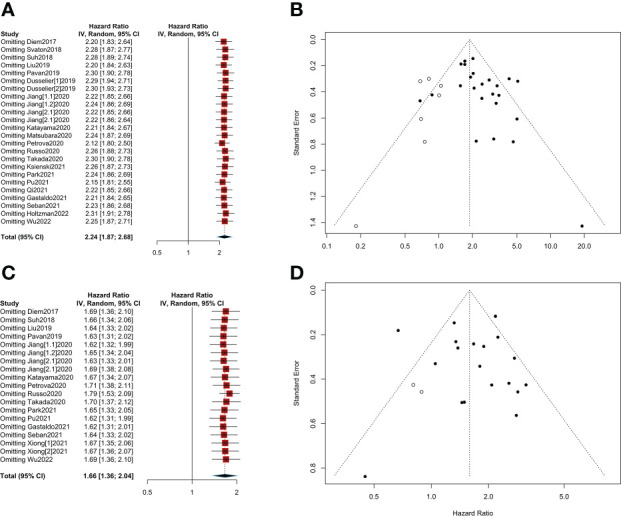
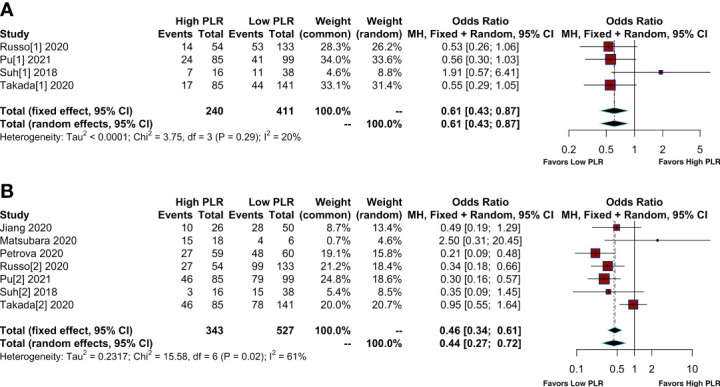
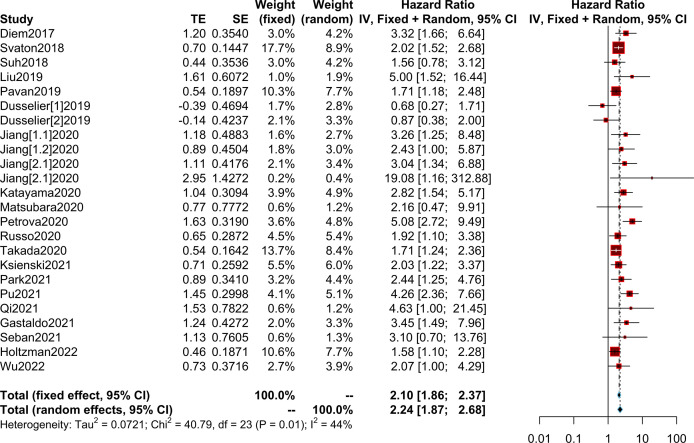
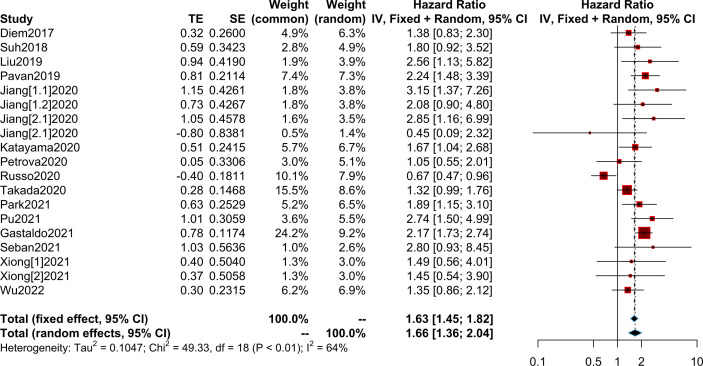
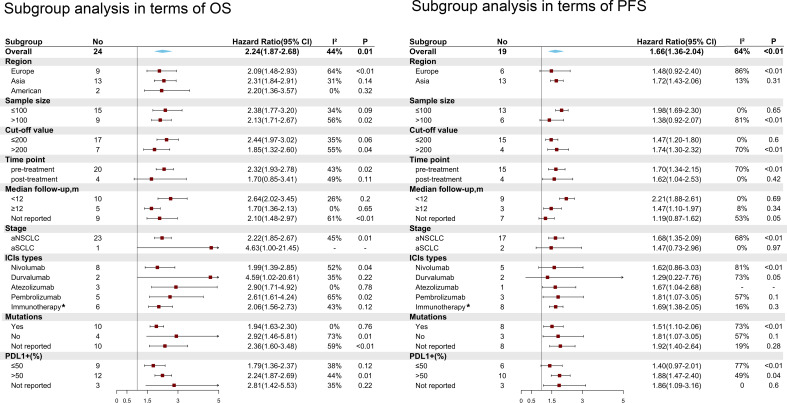
A total of 21 included studies involving 2312 patients with advanced lung cancer receiving immunotherapy were included. The combined results suggested that elevated PLR was associated with poorer OS (HR=2.24; 95% CI: 1.87-2.68; I² =44%; P=0.01) and PFS (HR=1.66; 95% CI: 1.36-2.04; I² =64%; P<0.01). Furthermore, elevated PLR showed a lower ORR (OR= 0.61; 95% CI: 0.43-0.87, I²=20%; P=0.29) and DCR (OR= 0.44; 95% CI: 0.27-0.72, I²=61%; P=0.02). In subgroup analyses, pretreatment PLR was significantly associated with adverse OS and PFS. The same results were observed in different PLRs in terms of cutoff value (>200 vs. ≤200). Furthermore, high PLR was significantly associated with poor OS and PFS in advanced non-small cell lung cancer (NSCLC); however, PLR was not associated with OS and PFS in advanced small cell lung cancer (SCLC). In addition, PLR predicted poor OS irrespective of regions and types of immune checkpoint inhibitors (ICIs).
On the whole, patients with low PLR had better OS and PFS, as well as higher ORR and DCR when receiving immunotherapy in advanced lung cancer especially for advanced NSCLC. And further investigations are warranted to confirm the prognostic value of PLR in advanced SCLC.
https://www.crd.york.ac.uk/PROSPERO/, identifier CRD42022315976.
血小板与淋巴细胞比值(PLR)是否可作为晚期肺癌免疫治疗疗效的潜在指标仍存在争议。本荟萃分析旨在解决这一问题。
截至2022年3月,我们检索了PubMed、Embase、Web of Science和Cochrane图书馆,以检索可能符合条件的文章。合并风险比(HR)和95%置信区间(CI)用于评估PLR与无进展生存期(PFS)以及总生存期(OS)之间的关系,而合并比值比(OR)和95%CI用于评估PLR与客观缓解率(ORR)以及疾病控制率(DCR)之间的关系。进一步进行亚组分析,以检测异质性来源以及PLR在不同组中关于OS和PFS的潜在预测价值。
共纳入21项研究,涉及2312例接受免疫治疗的晚期肺癌患者。合并结果表明,PLR升高与较差的OS(HR=2.24;95%CI:1.87-2.68;I² =44%;P=0.01)和PFS(HR=1.66;95%CI:1.36-2.04;I² =64%;P<0.01)相关。此外,PLR升高显示出较低的ORR(OR= 0.61;95%CI:0.43-0.87,I²=20%;P=0.29)和DCR(OR= 0.44;95%CI:0.27-0.72,I²=61%;P=0.02)。在亚组分析中,治疗前PLR与不良的OS和PFS显著相关。在不同的PLR临界值(>200 vs.≤200)方面观察到相同的结果。此外,高PLR与晚期非小细胞肺癌(NSCLC)较差的OS和PFS显著相关;然而,PLR与晚期小细胞肺癌(SCLC)的OS和PFS无关。此外,无论免疫检查点抑制剂(ICI)的区域和类型如何,PLR均预测OS较差。
总体而言,PLR较低的患者在接受晚期肺癌尤其是晚期NSCLC免疫治疗时,具有更好的OS和PFS,以及更高的ORR和DCR。有必要进一步研究以证实PLR在晚期SCLC中的预后价值。