Division of Psychiatry, University College London, 6th Floor Maple House, 149 Tottenham Court Road, London, W1T 7NF, UK.
Department of Psychology, Faculty of Psychology and Educational Sciences, University of Geneva, Geneva, Switzerland.
Alzheimers Res Ther. 2022 Sep 6;14(1):125. doi: 10.1186/s13195-022-01057-w.
Older individuals with subjective cognitive decline (SCD) perceive that their cognition has declined but do not show objective impairment on neuropsychological tests. Individuals with SCD are at elevated risk of objective cognitive decline and incident dementia. Non-pharmacological interventions (including mindfulness-based and health self-management approaches) are a potential strategy to maintain or improve cognition in SCD, which may ultimately reduce dementia risk.
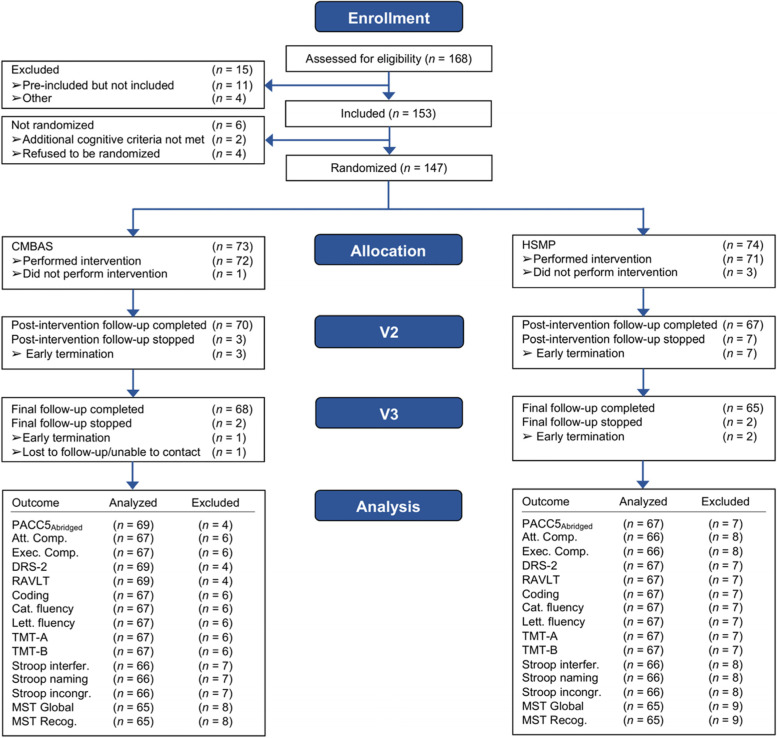
This study utilized data from the SCD-Well randomized controlled trial. One hundred forty-seven older adults with SCD (M = 72.7 years; 64% female) were recruited from memory clinics in four European countries and randomized to one of two group-based, 8-week interventions: a Caring Mindfulness-based Approach for Seniors (CMBAS) or a health self-management program (HSMP). Participants were assessed at baseline, post-intervention (week 8), and at 6-month follow-up (week 24) using a range of cognitive tests. From these tests, three composites were derived-an "abridged" Preclinical Alzheimer's Cognitive Composite 5 (PACC5), an attention composite, and an executive function composite. Both per-protocol and intention-to-treat analyses were performed. Linear mixed models evaluated the change in outcomes between and within arms and adjusted for covariates and cognitive retest effects. Sensitivity models repeated the per-protocol analyses for participants who attended ≥ 4 intervention sessions.
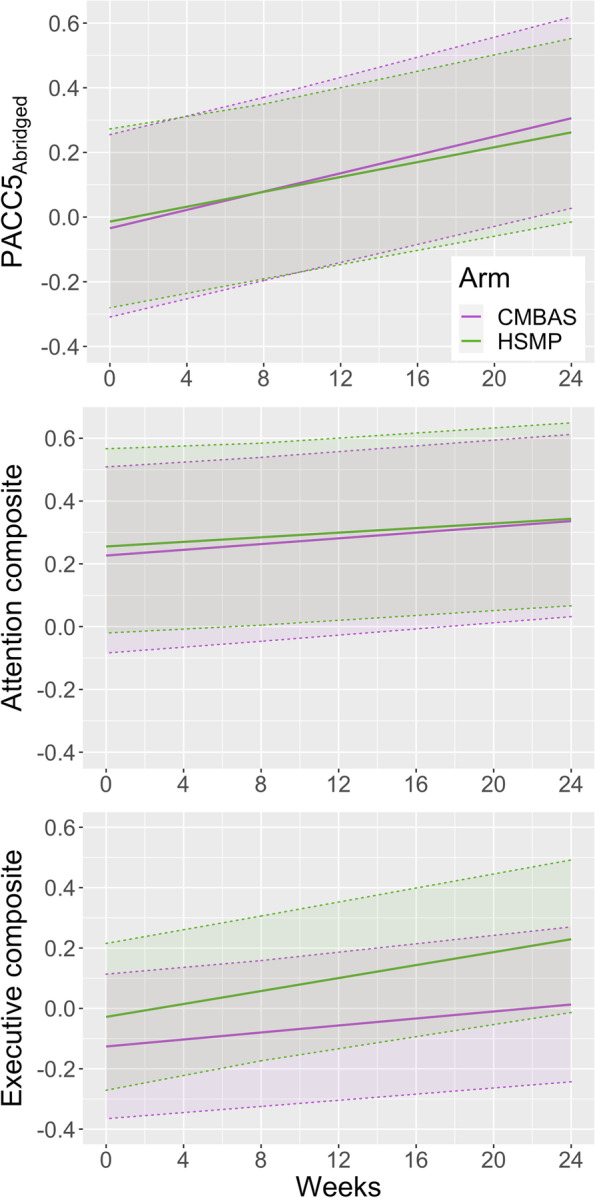
Across all cognitive composites, there were no significant time-by-trial arm interactions and no measurable cognitive retest effects; sensitivity analyses supported these results. Improvements, however, were observed within both trial arms on the PACC5 from baseline to follow-up (Δ [95% confidence interval]: CMBAS = 0.34 [0.19, 0.48]; HSMP = 0.30 [0.15, 0.44]). There was weaker evidence of an improvement in attention but no effects on executive function.
Two non-pharmacological interventions conferred small, non-differing improvements to a global cognitive composite sensitive to amyloid-beta-related decline. There was weaker evidence of an effect on attention, and no evidence of an effect on executive function. Importantly, observed improvements were maintained beyond the end of the interventions. Improving cognition is an important step toward dementia prevention, and future research is needed to delineate the mechanisms of action of these interventions and to utilize clinical endpoints (i.e., progression to mild cognitive impairment or dementia).
ClinicalTrials.gov, NCT03005652.
有主观认知下降(SCD)的老年人认为自己的认知能力下降,但在神经心理学测试中没有表现出客观损害。有 SCD 的个体有发生客观认知下降和出现痴呆的风险增加。非药物干预(包括基于正念和健康自我管理的方法)是维持或改善 SCD 认知的一种潜在策略,这可能最终降低痴呆风险。
本研究使用了 SCD-Well 随机对照试验的数据。从四个欧洲国家的记忆诊所招募了 147 名有 SCD 的老年人(M=72.7 岁;64%为女性),并将他们随机分为两组,每组 8 周的干预措施:老年人关怀正念方法(CMBAS)或健康自我管理方案(HSMP)。参与者在基线、干预后(第 8 周)和 6 个月随访(第 24 周)时使用一系列认知测试进行评估。从这些测试中,得出了三个综合测试:一个“简化”的临床前阿尔茨海默病认知综合测试 5(PACC5)、注意力综合测试和执行功能综合测试。对数据进行了意向性治疗和按方案分析。线性混合模型评估了试验臂之间和臂内的结果变化,并对协变量和认知复测效果进行了调整。敏感性分析针对参加了≥4 次干预的参与者重复了按方案分析。
在所有认知综合测试中,没有观察到时间与试验臂之间的交互作用,也没有可测量的认知复测效应;敏感性分析支持了这些结果。然而,在两个试验臂中,从基线到随访时,PACC5 都有改善(CMBAS=0.34[0.19,0.48];HSMP=0.30[0.15,0.44])。在注意力方面有较弱的改善证据,但在执行功能方面没有效果。
两种非药物干预措施对一种能敏感检测与淀粉样蛋白-β相关下降的全球认知综合测试产生了较小的、无差异的改善。在注意力方面有较弱的效果证据,而在执行功能方面没有证据。重要的是,观察到的改善在干预结束后仍得以维持。改善认知是预防痴呆的重要步骤,需要进一步研究来阐明这些干预措施的作用机制,并利用临床终点(即进展为轻度认知障碍或痴呆)。
ClinicalTrials.gov,NCT03005652。