Division of Radiology, Department of Medical Technology, Kyushu University Hospital, 3-1-1, Maidashi, Higashi-ku, Fukuoka, 812-8582, Japan.
Department of Medical Physics, Graduate School of Medical Sciences, Kindai University, 377-2, Ohno-Higashi, Osakasayama, Osaka, 589-8511, Japan.
Sci Rep. 2022 Sep 10;12(1):15282. doi: 10.1038/s41598-022-19498-6.
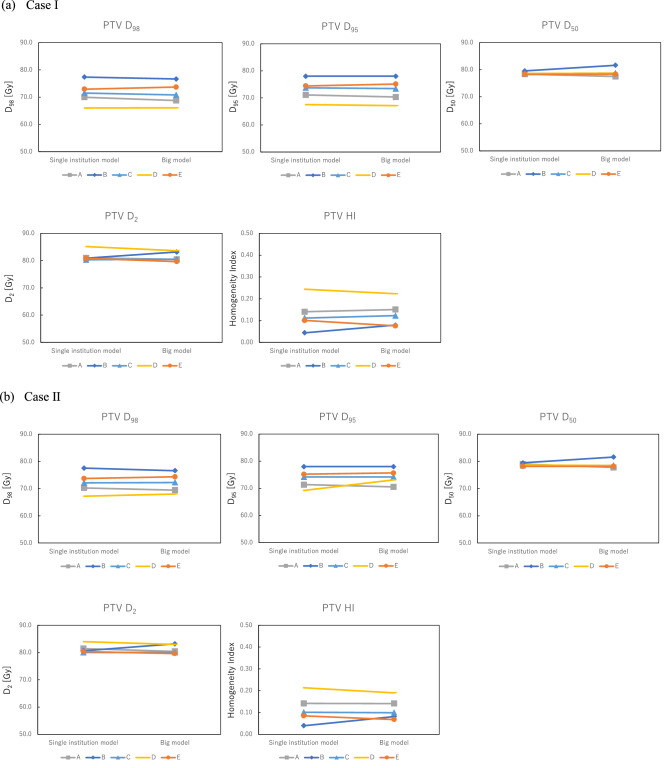
We established a multi-institution model (big model) of knowledge-based treatment planning with over 500 treatment plans from five institutions in volumetric modulated arc therapy (VMAT) for prostate cancer. This study aimed to clarify the efficacy of using a large number of registered treatment plans for sharing the big model. The big model was created with 561 clinically approved VMAT plans for prostate cancer from five institutions (A: 150, B: 153, C: 49, D: 60, and E: 149) with different planning strategies. The dosimetric parameters of planning target volume (PTV), rectum, and bladder for two validation VMAT plans generated with the big model were compared with those from each institutional model (single-institution model). The goodness-of-fit of regression lines (R and χ values) and ratios of the outliers of Cook's distance (CD) > 4.0, modified Z-score (mZ) > 3.5, studentized residual (SR) > 3.0, and areal difference of estimate (dA) > 3.0 for regression scatter plots in the big model and single-institution model were also evaluated. The mean ± standard deviation (SD) of dosimetric parameters were as follows (big model vs. single-institution model): 79.0 ± 1.6 vs. 78.7 ± 0.5 (D) and 0.13 ± 0.06 vs. 0.13 ± 0.07 (Homogeneity Index) for the PTV; 6.6 ± 4.0 vs. 8.4 ± 3.6 (V) and 32.4 ± 3.8 vs. 46.6 ± 15.4 (V) for the rectum; and 13.8 ± 1.8 vs. 13.3 ± 4.3 (V) and 39.9 ± 2.0 vs. 38.4 ± 5.2 (V) for the bladder. The R values in the big model were 0.251 and 0.755 for rectum and bladder, respectively, which were comparable to those from each institution model. The respective χ values in the big model were 1.009 and 1.002, which were closer to 1.0 than those from each institution model. The ratios of the outliers in the big model were also comparable to those from each institution model. The big model could generate a comparable VMAT plan quality compared with each single-institution model and therefore could possibly be shared with other institutions.
我们建立了一个基于多机构的知识型治疗计划模型(大模型),其中包含了 5 个机构的 500 多个容积旋转调强放疗(VMAT)治疗计划,用于前列腺癌治疗。本研究旨在阐明使用大量已注册的治疗计划来共享大模型的效果。该大模型是使用来自 5 个机构(A:150,B:153,C:49,D:60 和 E:149)的 561 个经临床批准的前列腺癌 VMAT 计划创建的,这些计划具有不同的计划策略。使用大模型生成的两个验证 VMAT 计划的计划靶区(PTV)、直肠和膀胱的剂量学参数与每个机构模型(单机构模型)进行了比较。对大模型和单机构模型中回归散点图的回归线的拟合优度(R 和 χ 值)以及 Cook 距离(CD)>4.0、修正 Z 分数(mZ)>3.5、学生化残差(SR)>3.0 和估计面积差(dA)>3.0 的离群值的比例进行了评估。大模型和单机构模型中剂量学参数的平均值±标准偏差(SD)如下:PTV:79.0±1.6 vs. 78.7±0.5(D)和 0.13±0.06 vs. 0.13±0.07(均匀性指数);直肠:6.6±4.0 vs. 8.4±3.6(V)和 32.4±3.8 vs. 46.6±15.4(V);膀胱:13.8±1.8 vs. 13.3±4.3(V)和 39.9±2.0 vs. 38.4±5.2(V)。大模型中直肠和膀胱的 R 值分别为 0.251 和 0.755,与各机构模型相当。大模型的 χ 值分别为 1.009 和 1.002,比各机构模型更接近 1.0。大模型中离群值的比例也与各机构模型相当。大模型可以生成与各单机构模型相当的 VMAT 计划质量,因此可以与其他机构共享。