Department of Radiology and Radiation Oncology, Niigata University Graduate School of Medical and Dental Sciences, Niigata, Japan.
Br J Radiol. 2022 Dec 1;95(1140):20220374. doi: 10.1259/bjr.20220374. Epub 2022 Sep 26.
To determine the added value of combining intratumoral and peritumoral CT radiomics for the prediction of epidermal growth factor receptor (EGFR) gene mutations in primary lung cancer (PLC).
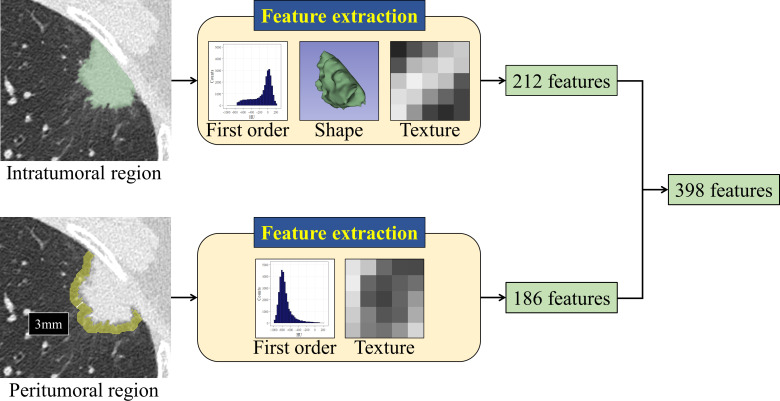
This study included 478 patients with PLC (348 adenocarcinomas and 130 other histological types) who underwent surgical resection and EGFR gene testing. Two radiologists performed segmentation of tumors and peritumoral regions using precontrast high-resolution CT images, and 398 radiomic features (212 intra- and 186 peritumoral features) were extracted. The peritumoral region was defined as the lung parenchyma within a distance of 3 mm from the tumor border. Model performance was estimated using Random Forest, a machine-learning algorithm.
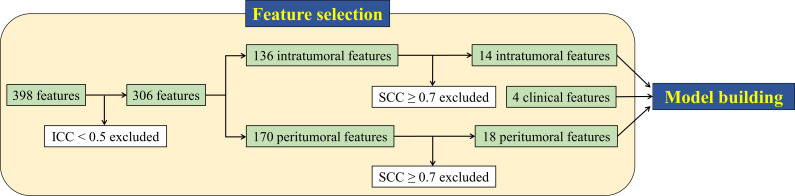
EGFR mutations were found in 162 tumors; 161 adenocarcinomas, and one pleomorphic carcinoma. After exclusion of poorly reproducible and redundant features, 32 radiomic features remained (14 intra- and 18 peritumoral features) and were included in the model building. For predicting EGFR mutations, combining intra- and peritumoral radiomics significantly improved the performance compared to intratumoral radiomics alone (AUC [area under the receiver operating characteristic curve], 0.774 0.730; < 0.001). Even in adenocarcinomas only, adding peritumoral radiomics significantly increased performance (AUC, 0.687 0.630; < 0.001). The predictive performance using radiomics and clinical features was significantly higher than that of clinical features alone (AUC, 0.826 0.777; = 0.005).
Combining intra- and peritumoral radiomics improves the predictive accuracy of EGFR mutations and could be used to aid in decision-making of whether to perform biopsy for gene tests.
Adding peritumoral to intratumoral radiomics yields greater accuracy than intratumoral radiomics alone in predicting EGFR mutations and may serve as a non-invasive method of predicting of the gene status in PLC.
确定联合肿瘤内和肿瘤周围 CT 放射组学预测原发性肺癌(PLC)中表皮生长因子受体(EGFR)基因突变的附加值。
本研究纳入了 478 名接受手术切除和 EGFR 基因检测的 PLC 患者(348 例腺癌和 130 例其他组织学类型)。两名放射科医生使用对比前高分辨率 CT 图像对肿瘤和肿瘤周围区域进行分割,并提取 398 个放射组学特征(212 个肿瘤内特征和 186 个肿瘤周围特征)。肿瘤周围区域定义为距离肿瘤边界 3mm 范围内的肺实质。使用机器学习算法随机森林估计模型性能。
在 162 个肿瘤中发现了 EGFR 突变;161 例腺癌和 1 例多形性癌。排除重现性差和冗余特征后,仍有 32 个放射组学特征(14 个肿瘤内特征和 18 个肿瘤周围特征)纳入模型构建。与仅肿瘤内放射组学相比,联合肿瘤内和肿瘤周围放射组学显著提高了预测 EGFR 突变的性能(AUC [受试者工作特征曲线下的面积],0.774 vs. 0.730;<0.001)。即使在腺癌中,添加肿瘤周围放射组学也显著提高了性能(AUC,0.687 vs. 0.630;<0.001)。使用放射组学和临床特征的预测性能明显高于仅使用临床特征的预测性能(AUC,0.826 vs. 0.777;=0.005)。
联合肿瘤内和肿瘤周围放射组学提高了 EGFR 突变的预测准确性,并可用于辅助决定是否进行基因检测活检。
在预测 EGFR 突变方面,肿瘤内放射组学与肿瘤周围放射组学联合应用的准确性高于单独使用肿瘤内放射组学,可能成为预测 PLC 基因状态的一种非侵入性方法。