Gérard Alexandre O, Barbosa Susana, Parassol Nadège, Andreani Marine, Merino Diane, Cremoni Marion, Laurain Audrey, Pinel Sylvine, Bourneau-Martin Delphine, Rocher Fanny, Esnault Vincent L M, Borchiellini Delphine, Sicard Antoine, Drici Milou-Daniel
Department of Nephrology-Dialysis-Transplantation, University Hospital Centre of Nice, Nice, France.
Department of Pharmacology and Pharmacovigilance Centre of Nice, University Hospital Centre of Nice, Nice, France.
Clin Kidney J. 2022 Apr 28;15(10):1881-1887. doi: 10.1093/ckj/sfac109. eCollection 2022 Oct.
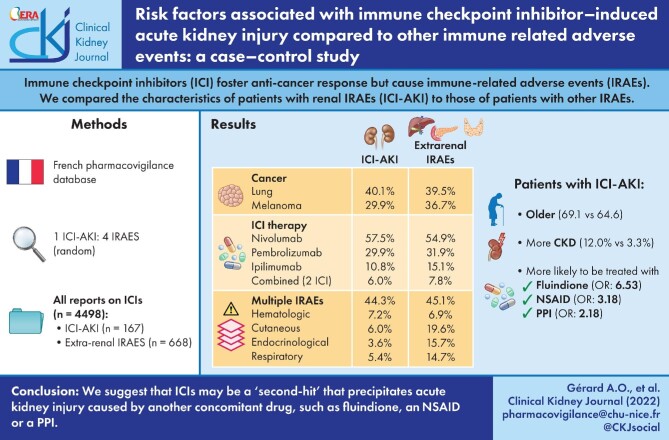
Immune checkpoint inhibitors (ICIs) foster anti-cancer immune responses. Their efficacy comes at the cost of immune-related adverse events (IRAEs). The latter affects various organs, including kidneys, mostly as acute tubulointerstitial nephritis, the pathophysiology of which remains unclear. We conducted a multicentre case-control study to compare the characteristics of patients with renal IRAEs (ICI-AKI) with those of patients diagnosed with other IRAEs.
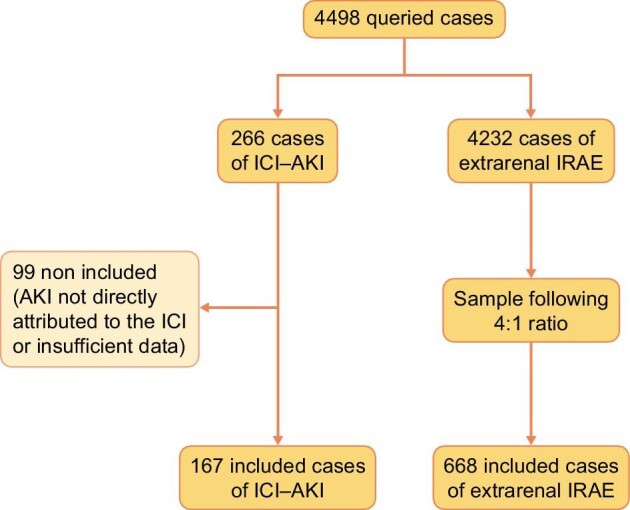
We queried the French pharmacovigilance database for all adverse events involving ICIs. Reports were classified as ICI-AKI or extrarenal IRAE. For each ICI-AKI report, four reports of extrarenal IRAEs were randomly included (control group, 4:1 ratio). Variables showing an association with a P < 0.05 were included as covariates in a multivariate analysis.
Therefore, 167 ICI-AKI reports were compared with 668 extrarenal IRAEs. At least one concomitant extrarenal IRAE was mentioned in 44.3% of ICI-AKI reports. Patients with ICI-AKI were significantly older than patients with extrarenal IRAEs (69.1 versus 64.6 years; P = 0.0135), and chronic kidney disease was significantly more prevalent (12.0% versus 3.3%; P = 0.0125). Patients with ICI-AKI were significantly more likely to be treated with fluindione [adjusted odds ratio (OR) 6.53, 95% confidence interval (95% CI) 2.21-19.31; P = 0.0007], a non-steroidal anti-inflammatory drug (NSAID, OR 3.18, 95% CI 1.07-9.4; P = 0.0368) or a proton-pump inhibitor (PPI, OR 2.18, 95% CI 1.42-3.34; P = 0.0004).
This study is limited by a lack of data, preventing confirmation of numerous reports therefore not included in the analysis. We are unable to draw definite pathophysiological conclusions from our data. Nonetheless, we suggest that ICIs may be a 'second-hit' that precipitates acute kidney injury caused by another concomitant drug (fluindione, NSAID or PPI).
免疫检查点抑制剂(ICI)可促进抗癌免疫反应。其疗效是以免疫相关不良事件(IRAEs)为代价的。后者会影响包括肾脏在内的各种器官,主要表现为急性肾小管间质性肾炎,其病理生理学仍不清楚。我们进行了一项多中心病例对照研究,以比较发生肾脏IRAEs(ICI-AKI)的患者与被诊断为其他IRAEs的患者的特征。
我们在法国药物警戒数据库中查询了所有涉及ICI的不良事件。报告被分类为ICI-AKI或肾外IRAEs。对于每一份ICI-AKI报告,随机纳入四份肾外IRAEs报告(对照组,比例为4:1)。在多变量分析中,将显示P<0.05关联的变量作为协变量纳入。
因此,将167份ICI-AKI报告与668份肾外IRAEs报告进行了比较。44.3%的ICI-AKI报告中提到至少有一种伴随的肾外IRAEs。发生ICI-AKI的患者明显比发生肾外IRAEs的患者年龄大(69.1岁对64.6岁;P = 0.0135),慢性肾脏病的患病率明显更高(12.0%对3.3%;P = 0.0125)。发生ICI-AKI的患者使用氟茚二酮[调整后的优势比(OR)6.53,95%置信区间(95%CI)2.21-19.31;P = 0.0007]、非甾体抗炎药(NSAID,OR 3.18,95%CI 1.07-9.4;P = 0.0368)或质子泵抑制剂(PPI,OR 2.18,95%CI 1.42-3.34;P = 0.0004)治疗的可能性明显更高。
本研究因缺乏数据而受到限制,无法证实因此未纳入分析的众多报告。我们无法从我们的数据中得出明确的病理生理学结论。尽管如此,我们认为ICI可能是引发由另一种伴随药物(氟茚二酮、NSAID或PPI)导致的急性肾损伤的“二次打击”因素。