Sun Dawei, Liu Juan, Wang Yunfang, Dong Jiahong
Department of Hepatobiliary and Pancreatic Surgery, The First Hospital of Jilin University, Changchun, China.
Hepato-Pancreato-Biliary Centre, Beijing Tsinghua Changgung Hospital, Tsinghua University, Beijing, China.
Front Oncol. 2022 Sep 8;12:944537. doi: 10.3389/fonc.2022.944537. eCollection 2022.
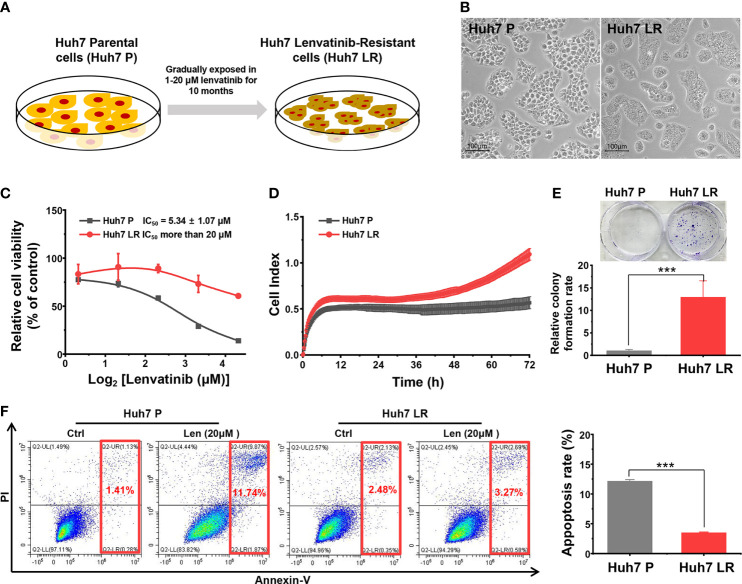
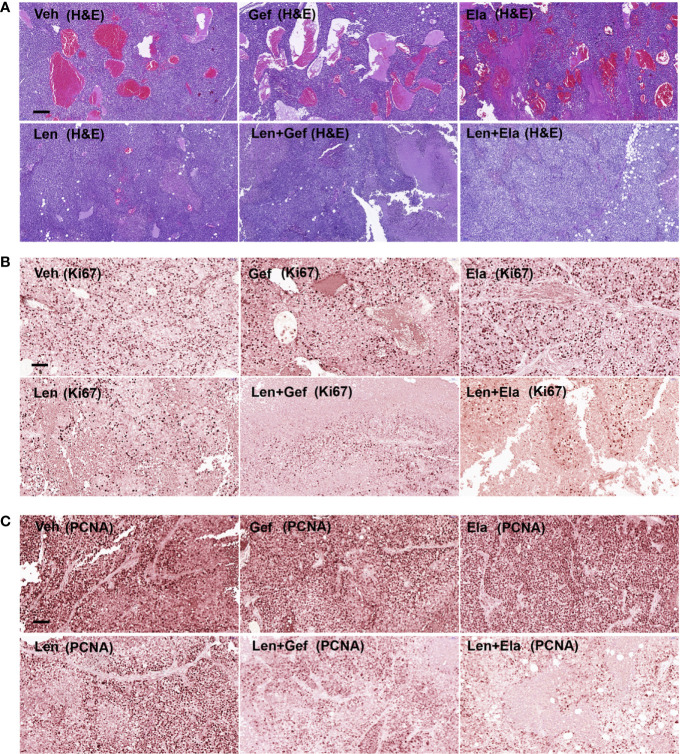
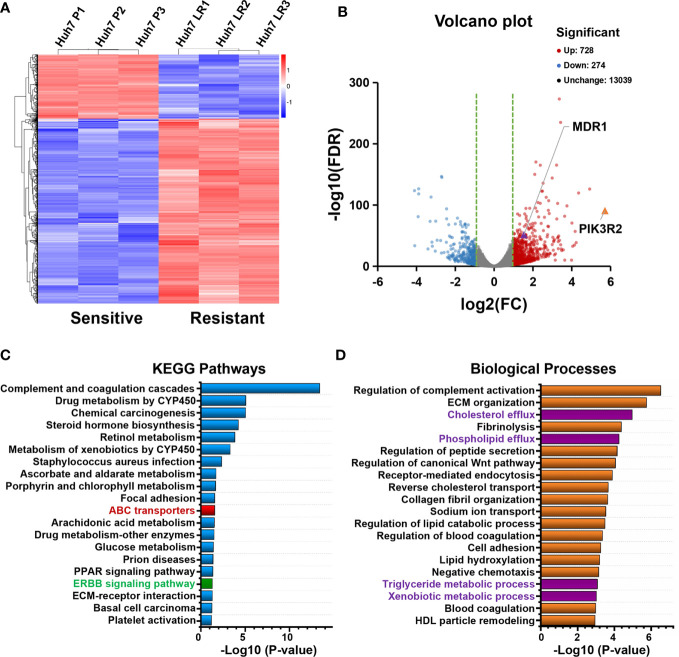
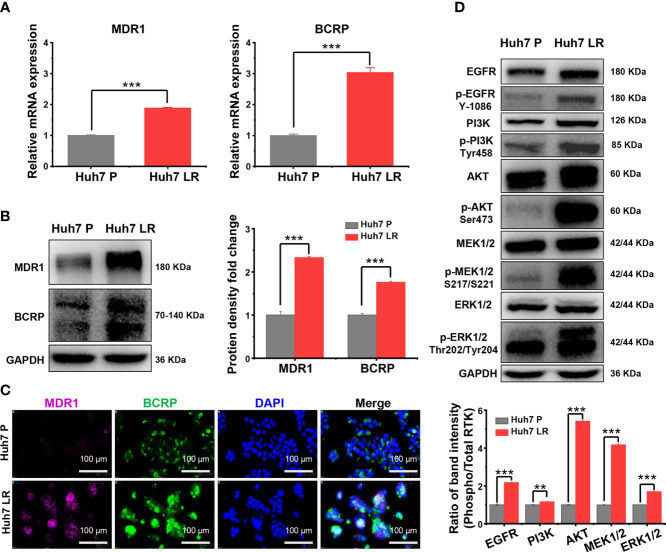
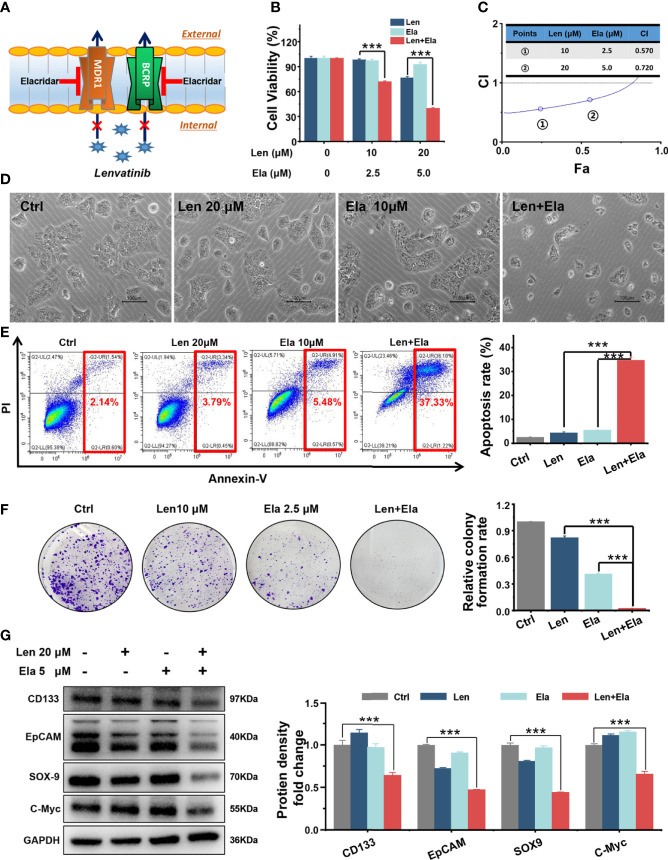
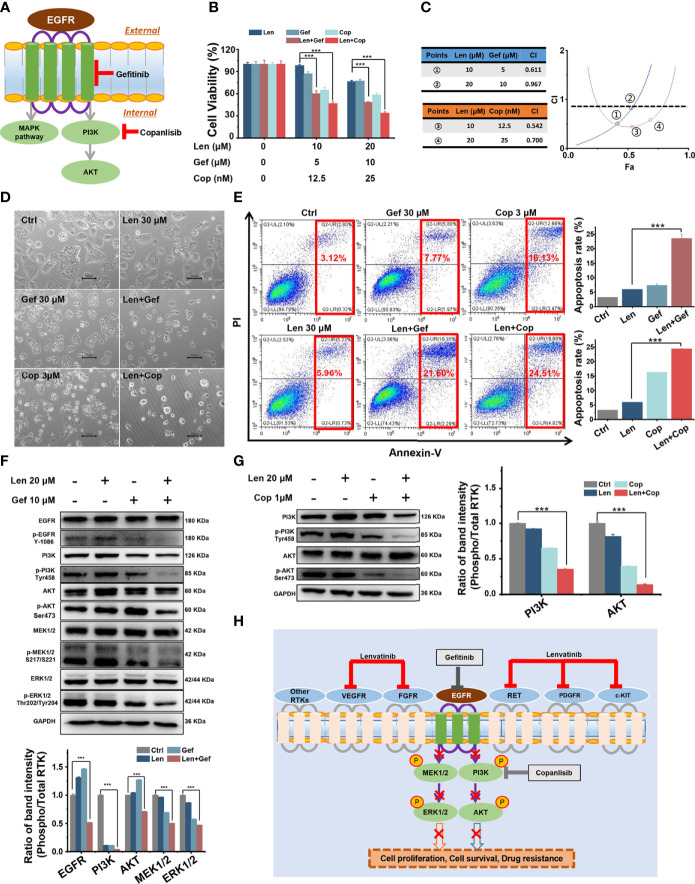
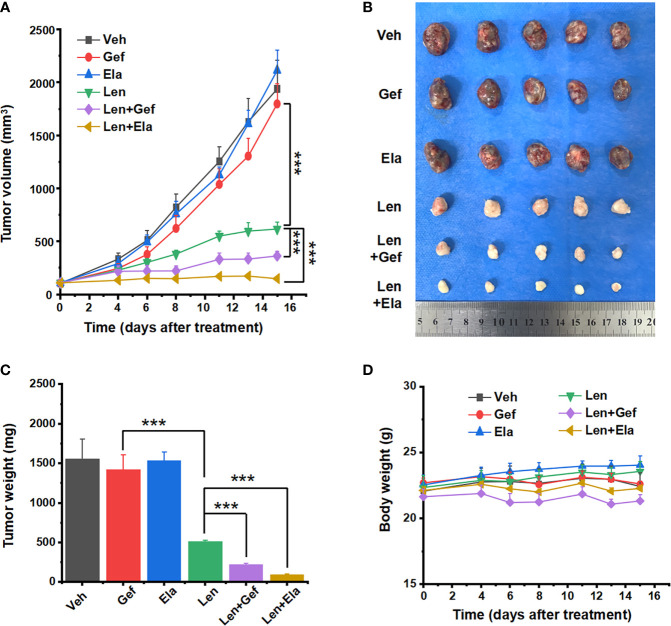
Lenvatinib is the first-line treatment for hepatocellular carcinoma (HCC), the most common type of primary liver cancer; however, some patients become refractory to lenvatinib. The underlying mechanism of lenvatinib resistance (LR) in patients with advanced HCC remains unclear. We focused on exploring the potential mechanism of LR and novel treatments of lenvatinib-resistant HCC. In particular, we established a Huh7 LR cell line and performed , bioinformatic, and biochemical assays. Additionally, we used a Huh7-LR cell-derived xenograft mouse model to confirm the results . Following LR induction, multidrug resistance protein 1 (MDR1) and breast cancer resistance protein (BCRP) transporters were markedly upregulated, and the epidermal growth factor receptor (EGFR), MEK/ERK, and PI3K/AKT pathways were activated. , the co-administration of elacridar, a dual MDR1 and BCRP inhibitor, with lenvatinib inhibited proliferation and induced apoptosis of LR cells. These effects might be due to inhibiting cancer stem-like cells (CSCs) properties, by decreasing colony formation and downregulating CD133, EpCAM, SOX-9, and c-Myc expression. Moreover, the co-administration of gefitinib, an EGFR inhibitor, with lenvatinib retarded proliferation and induced apoptosis of LR cells. These similar effects might be caused by the inhibition of EGFR-mediated MEK/ERK and PI3K/AKT pathway activation. , co-administration of lenvatinib with elacridar or gefitinib suppressed tumour growth and angiogenesis. Therefore, inhibiting MDR1 and BCRP transporters or targeting the EGFR/PI3K pathway might overcome LR in HCC. Notably, lenvatinib should be used to treat HCC after LR induction owing to its role in inhibiting tumour proliferation and angiogenesis. Our findings could help develop novel and effective treatment strategies for HCC.
乐伐替尼是最常见的原发性肝癌——肝细胞癌(HCC)的一线治疗药物;然而,一些患者会对乐伐替尼产生耐药性。晚期HCC患者中乐伐替尼耐药(LR)的潜在机制仍不清楚。我们专注于探索LR的潜在机制以及乐伐替尼耐药HCC的新治疗方法。具体而言,我们建立了Huh7 LR细胞系并进行了生物信息学和生化分析。此外,我们使用Huh7-LR细胞衍生的异种移植小鼠模型来证实结果。在诱导LR后,多药耐药蛋白1(MDR1)和乳腺癌耐药蛋白(BCRP)转运体明显上调,表皮生长因子受体(EGFR)、MEK/ERK和PI3K/AKT通路被激活。此外,双重MDR1和BCRP抑制剂艾拉司群与乐伐替尼联合给药可抑制LR细胞的增殖并诱导其凋亡。这些作用可能是由于通过减少集落形成和下调CD133、EpCAM、SOX-9和c-Myc的表达来抑制癌症干细胞(CSC)特性。此外,EGFR抑制剂吉非替尼与乐伐替尼联合给药可抑制LR细胞的增殖并诱导其凋亡。这些相似的作用可能是由于抑制了EGFR介导的MEK/ERK和PI3K/AKT通路激活。因此,乐伐替尼与艾拉司群或吉非替尼联合给药可抑制肿瘤生长和血管生成。因此,抑制MDR1和BCRP转运体或靶向EGFR/PI3K通路可能克服HCC中的LR。值得注意的是,由于乐伐替尼在抑制肿瘤增殖和血管生成中的作用,应在诱导LR后用于治疗HCC。我们的研究结果有助于开发针对HCC的新型有效治疗策略。