Singh Prashant Kumar, Singh Lucky, Wehrmeister Fernando C, Singh Nishikant, Kumar Chandan, Singh Ankur, Sinha Dhirendra N, Bhutta Zulfiqar A, Singh Shalini
Division of Preventive Oncology & Population Health, WHO FCTC Knowledge Hub on Smokeless Tobacco, ICMR-National Institute of Cancer Prevention and Research, Noida, India.
ICMR - National Institute of Medical Statistics, New Delhi, India.
EClinicalMedicine. 2022 Sep 18;53:101660. doi: 10.1016/j.eclinm.2022.101660. eCollection 2022 Nov.
Smoking and smokeless tobacco use during the postpartum period is well studied in high-income countries, whereas low-income and middle-income countries (LMICs) lack evidence.
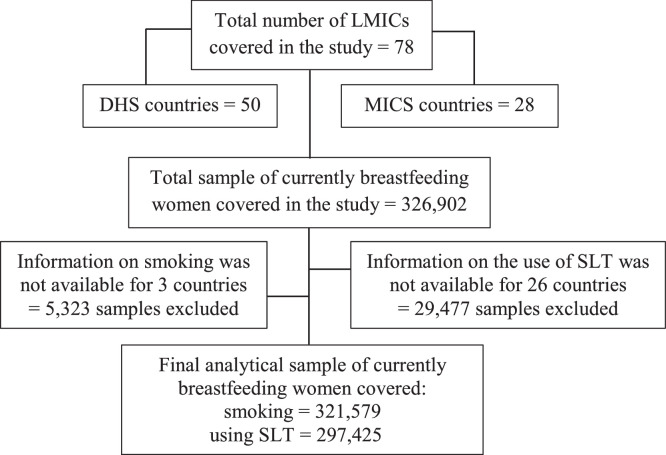
In this cross-sectional study we used data from the Demographic and Health Surveys (DHS) and Multiple Indicator Cluster Surveys (MICS) conducted in 78 LMICs between January 2010 and December 2019 to study tobacco use among 0.32 million sample lactating women. Age-standardized prevalence of smoking and smokeless tobacco use was estimated and presented with a 95% Confidence Interval (CI) for 78 LMICs. Pooled estimates overall and by WHO regions were obtained using random-effects meta-analyses. Country-level and community-level variance to understand contextual factors was also quantified using multilevel modelling.
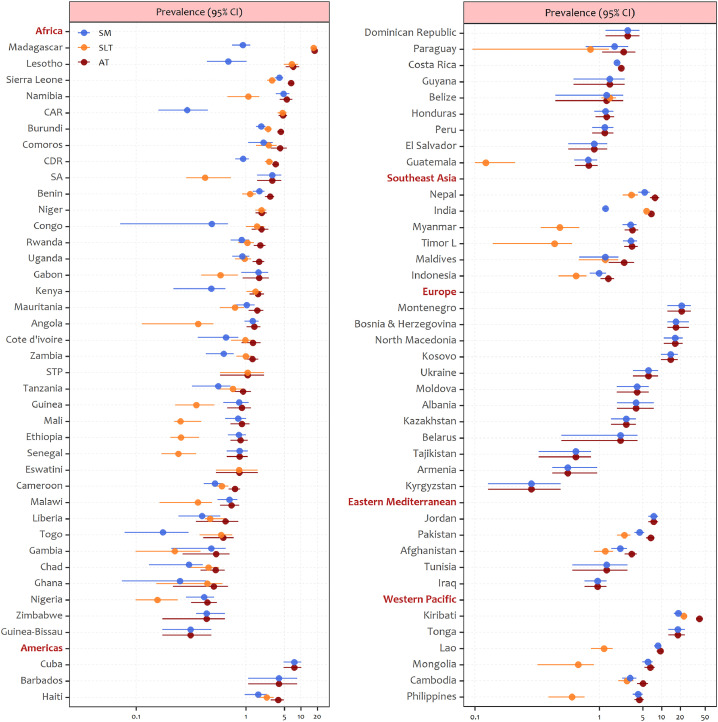
Pooled prevalence of any tobacco use among breastfeeding women in LMICs was 3.61% (95% CI 3.53-3.70); with the lowest prevalence in regions of the Americas (1.44%, 1.26-1.63) and the highest in the Southeast Asia region (6.13%, 6.0-6.27). The pooled prevalence of tobacco smoking was reported to be 1.16% (1.11-1.21), with the highest prevalence in the Eastern Mediterranean region (4.27%, 3.88-4.67) and the lowest in the African region (0.81%, 0.76-0.86). The pooled prevalence of smokeless tobacco use was reported to be 2.56% (2.49-2.63), with the highest prevalence in the Southeast Asia region (4.92%, 4.80-5.04). Illiterate and poor women in LMICs bore the enormous burden of tobacco use.
The prevalence of smoking and smokeless tobacco use among lactating women in LMICs varied considerably across different WHO regions. Considering the cross-sectional design of the study, caution is required while interpreting the results. To improve mothers' and children's health and nutrition outcomes and reduce health inequalities in LMICs, reducing tobacco use through evidence-based interventions is critical.
None.
高收入国家对产后吸烟和使用无烟烟草的情况进行了充分研究,而低收入和中等收入国家(LMICs)则缺乏相关证据。
在这项横断面研究中,我们使用了2010年1月至2019年12月期间在78个低收入和中等收入国家进行的人口与健康调查(DHS)和多指标类集调查(MICS)的数据,以研究32万例样本哺乳期妇女的烟草使用情况。估计了吸烟和使用无烟烟草的年龄标准化患病率,并给出了78个低收入和中等收入国家的95%置信区间(CI)。使用随机效应荟萃分析获得总体和按世卫组织区域的汇总估计值。还使用多水平模型对国家层面和社区层面的差异进行了量化,以了解背景因素。
低收入和中等收入国家母乳喂养妇女中任何烟草使用的汇总患病率为3.61%(95%CI 3.53 - 3.70);美洲地区患病率最低(1.44%,1.26 - 1.63),东南亚地区患病率最高(6.13%,6.0 - 6.27)。据报告,吸烟的汇总患病率为1.16%(1.11 - 1.21),东地中海地区患病率最高(4.27%,3.88 - 4.67),非洲地区患病率最低(0.81%,0.76 - 0.86)。据报告,使用无烟烟草的汇总患病率为2.56%(2.49 - 2.63),东南亚地区患病率最高(4.92%,4.80 - 5.04)。低收入和中等收入国家的文盲妇女和贫困妇女承受着巨大的烟草使用负担。
低收入和中等收入国家哺乳期妇女吸烟和使用无烟烟草的患病率在不同世卫组织区域差异很大。考虑到研究的横断面设计,在解释结果时需要谨慎。为改善低收入和中等收入国家母亲和儿童的健康及营养状况并减少健康不平等现象,通过循证干预减少烟草使用至关重要。
无。