Center for Immuno-Oncology, Center for Cancer Research, National Cancer Institute, National Institutes of Health, Bethesda, MD, United States.
Front Immunol. 2022 Sep 8;13:993624. doi: 10.3389/fimmu.2022.993624. eCollection 2022.
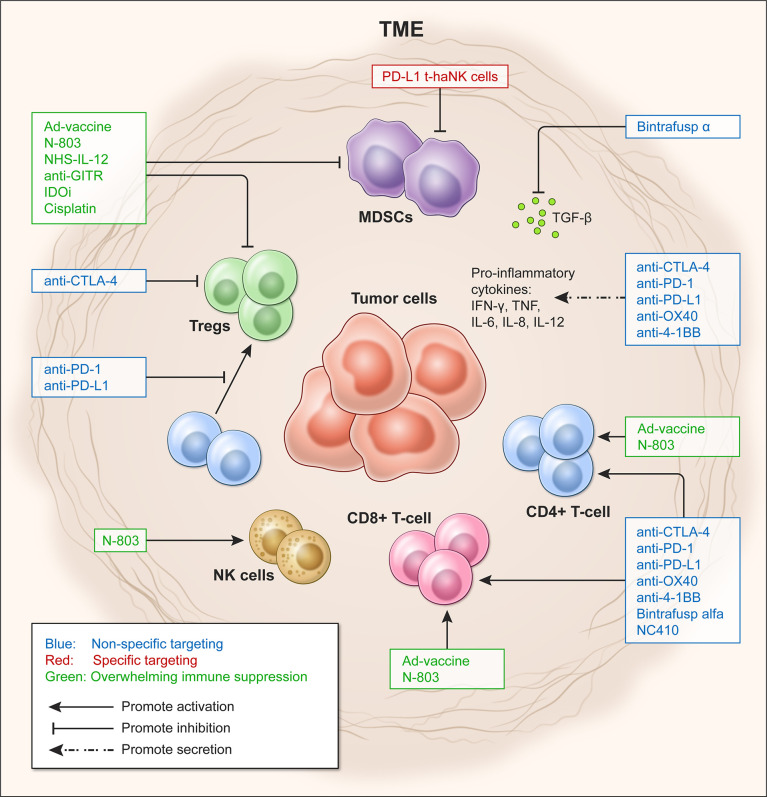
Immunotherapy has emerged as an effective therapeutic approach for several cancer types. However, only a subset of patients exhibits a durable response due in part to immunosuppressive mechanisms that allow tumor cells to evade destruction by immune cells. One of the hallmarks of immune suppression is the paucity of tumor-infiltrating lymphocytes (TILs), characterized by low numbers of effector CD4+ and CD8+ T cells in the tumor microenvironment (TME). Additionally, the proper activation and function of lymphocytes that successfully infiltrate the tumor are hampered by the lack of co-stimulatory molecules and the increase in inhibitory factors. These contribute to the imbalance of effector functions by natural killer (NK) and T cells and the immunosuppressive functions by myeloid-derived suppressor cells (MDSCs) and regulatory T cells (Tregs) in the TME, resulting in a dysfunctional anti-tumor immune response. Therefore, therapeutic regimens that elicit immune responses and reverse immune dysfunction are required to counter immune suppression in the TME and allow for the re-establishment of proper immune surveillance. Immuno-oncology (IO) agents, such as immune checkpoint blockade and TGF-β trapping molecules, have been developed to decrease or block suppressive factors to enable the activity of effector cells in the TME. Therapeutic agents that target immunosuppressive cells, either by direct lysis or altering their functions, have also been demonstrated to decrease the barrier to effective immune response. Other therapies, such as tumor antigen-specific vaccines and immunocytokines, have been shown to activate and improve the recruitment of CD4+ and CD8+ T cells to the tumor, resulting in improved T effector to Treg ratio. The preclinical data on these diverse IO agents have led to the development of ongoing phase I and II clinical trials. This review aims to provide an overview of select therapeutic strategies that tip the balance from immunosuppression to immune activity in the TME.
免疫疗法已成为多种癌症类型的有效治疗方法。然而,只有一部分患者表现出持久的反应,部分原因是免疫抑制机制允许肿瘤细胞逃避免疫细胞的破坏。免疫抑制的一个标志是肿瘤浸润淋巴细胞(TILs)的缺乏,其特征是肿瘤微环境(TME)中效应性 CD4+和 CD8+T 细胞数量低。此外,成功浸润肿瘤的淋巴细胞的适当激活和功能受到共刺激分子的缺乏和抑制因子的增加的阻碍。这些导致自然杀伤(NK)和 T 细胞的效应功能失衡以及髓源抑制细胞(MDSC)和调节性 T 细胞(Treg)的免疫抑制功能失衡,导致抗肿瘤免疫反应功能失调。因此,需要引发免疫反应并逆转免疫功能障碍的治疗方案来对抗 TME 中的免疫抑制作用,并允许重新建立适当的免疫监视。免疫肿瘤学(IO)药物,如免疫检查点阻断和 TGF-β捕获分子,已经被开发出来以减少或阻断抑制因子,从而使 TME 中的效应细胞发挥作用。靶向免疫抑制细胞的治疗药物,无论是通过直接溶解还是改变其功能,也已被证明可以降低有效免疫反应的障碍。其他疗法,如肿瘤抗原特异性疫苗和免疫细胞因子,已被证明可以激活和改善 CD4+和 CD8+T 细胞向肿瘤的募集,从而改善 T 效应细胞与 Treg 细胞的比例。这些不同的 IO 药物的临床前数据已经导致了正在进行的 I 期和 II 期临床试验的发展。这篇综述旨在提供对选择治疗策略的概述,这些策略可以使 TME 中的免疫抑制向免疫活性倾斜。