Jayasinghe Dilki, Nufer Kaitlin L, Betz-Stablein Brigid, Soyer H Peter, Janda Monika
Centre for Health Services Research, Faculty of Medicine, The University of Queensland, Brisbane, QLD, Australia.
Dermatology Research Centre, The University of Queensland Diamantina Institute, The University of Queensland, Brisbane, QLD, Australia.
Dermatol Ther (Heidelb). 2022 Nov;12(11):2453-2488. doi: 10.1007/s13555-022-00806-x. Epub 2022 Sep 30.
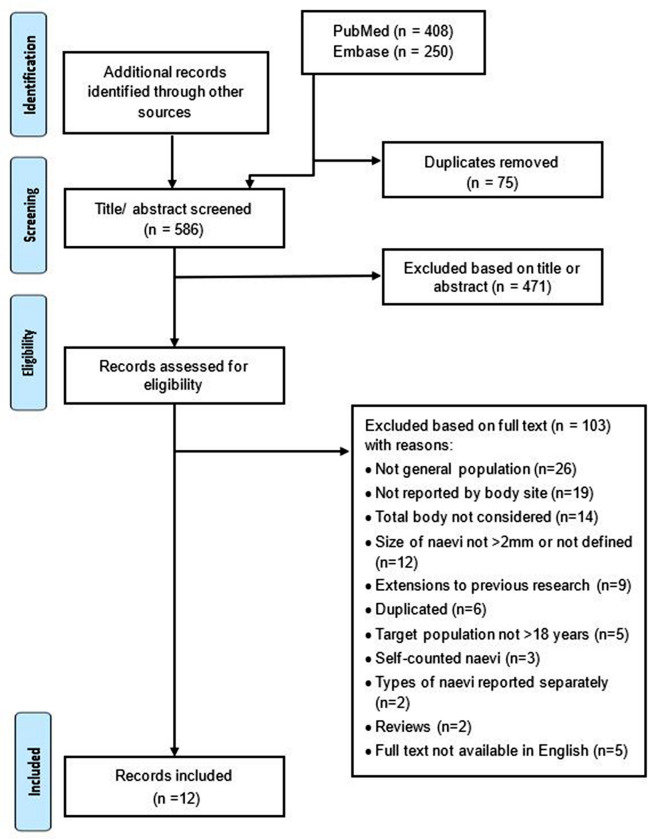
The number of melanocytic naevi is a major risk factor for melanoma. The divergent pathway hypothesis proposes that the propensity for naevus proliferation and malignant transformation may differ by body site and exposure to ultraviolet (UV) radiation. This scoping review aimed to summarise the evidence on the number and distribution of naevi (≥ 2 mm) on the body overall and by individual anatomical sites in Caucasian adults, and to assess whether studies used the International Agency for Research on Cancer (IARC) protocol to guide naevus counting processes. Systematic searches of Embase and PubMed identified 661 potentially relevant studies, and 12 remained eligible after full-text review. Studies varied widely in their counting protocols, reporting of naevus counts overall and by body sites, and used counting personnel with differing qualifications. Only one study used the IARC protocol. Studies reported that the highest number of naevi was on the trunk in males and on the arms in females. Body sites which receive intermittent exposure to UV radiation had higher density of naevi. Larger naevi (≥ 5 mm) were detected mostly on body sites intermittently exposed to UV radiation, and smaller naevi (< 5 mm) on chronically exposed sites. Studies reported that environmental and behavioural aspects related to UV radiation exposure, as well as genetic factors, all impact body site and size distribution of naevi. This review found that to overcome limitations of the current evidence, future studies should use consistent naevus counting protocols. Skin surface imaging could improve the reliability of findings. An updated IARC protocol is required that integrates these emerging standards and technologies to guide reliable and reproducible naevus counting in the future.
黑素细胞痣的数量是黑色素瘤的一个主要风险因素。分歧途径假说提出,痣增殖和恶性转化的倾向可能因身体部位和紫外线(UV)辐射暴露情况而异。本综述旨在总结白种人成年人全身及各个解剖部位≥2毫米痣的数量和分布的证据,并评估研究是否使用国际癌症研究机构(IARC)的方案来指导痣的计数过程。对Embase和PubMed进行系统检索,共识别出661项潜在相关研究,经过全文审查后,12项研究符合纳入标准。这些研究在计数方案、总体及各身体部位痣计数的报告方式以及计数人员资质方面差异很大。只有一项研究使用了IARC方案。研究报告称,男性痣数量最多的部位是躯干,女性是手臂。间歇性暴露于紫外线辐射的身体部位痣密度更高。较大的痣(≥5毫米)大多出现在间歇性暴露于紫外线辐射的身体部位,较小的痣(<5毫米)出现在长期暴露的部位。研究报告称,与紫外线辐射暴露相关的环境和行为因素以及遗传因素,都会影响痣的身体部位和大小分布。本综述发现,为克服现有证据的局限性,未来研究应采用一致的痣计数方案。皮肤表面成像可提高研究结果的可靠性。需要更新IARC方案,整合这些新出现的标准和技术,以指导未来可靠且可重复的痣计数。