Tang Yiyang, Chen Qin, Liang Benhui, Peng Baohua, Wang Meijuan, Sun Jing, Liu Zhenghui, Zha Lihuang, Yu Zaixin
Department of Cardiology, Xiangya Hospital, Central South University, Changsha, China.
Department of Neurology, Xiangya Hospital, Central South University, Changsha, China.
Front Cardiovasc Med. 2022 Sep 16;9:999391. doi: 10.3389/fcvm.2022.999391. eCollection 2022.
Coagulation disorder in congestive heart failure (CHF) has been well-documented. The prognostic value of a composite coagulation disorder score, which combines the absolute platelet count, international normalized ratio (INR), and activated partial thromboplastin time (APTT), has not been assessed in CHF. The present study endeavored to explore the association between the coagulation disorder score and adverse outcomes of critically ill patients with CHF.
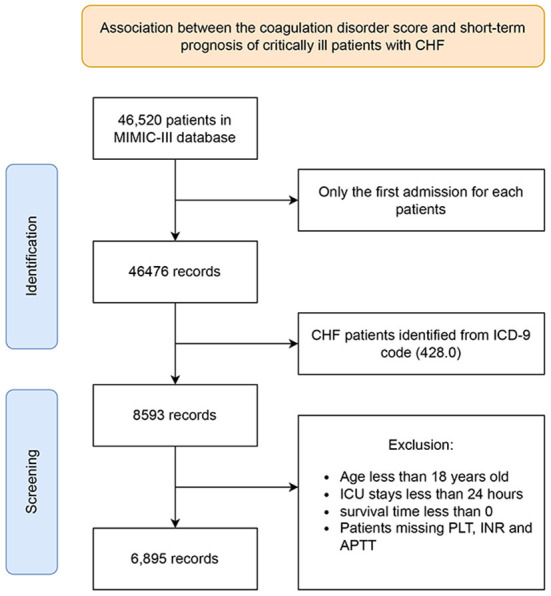
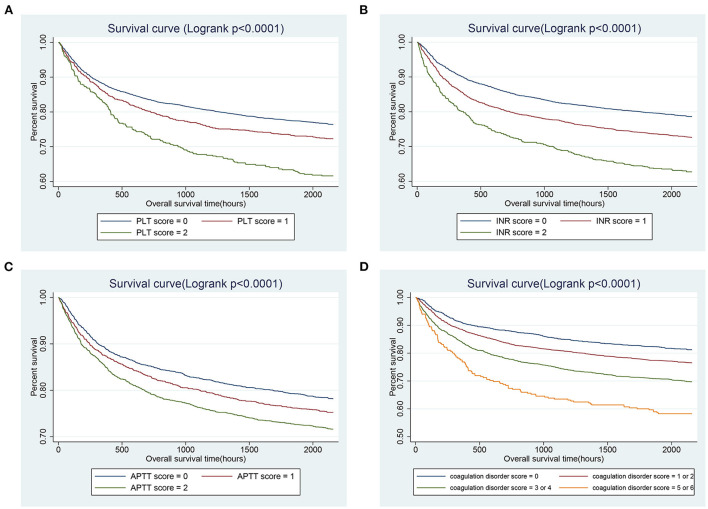
Patients diagnosed with CHF in the Medical Information Mart for Intensive Care III (MIMIC-III) database were included in the present retrospective cohort study. The coagulation disorder score was calculated according to the abnormalities of the absolute platelet count, INR, and APTT within 24 h after intensive care unit admission. The primary outcomes were the short-term all-cause mortality, including 30-, 90-day and in-hospital mortalities. The Kaplan-Meier (K-M) survival curve and the Cox proportional hazard model were performed to assess the correlation between coagulation disorder score and outcome events.
A total of 6,895 patients were enrolled in this study and divided into four groups according to the coagulation disorder score. K-M survival curve preliminarily indicated that subjects with higher coagulation disorder score presented lower survival rate and shorter survival time. After adjustment for potential confounders, the multivariate Cox analysis further illustrated that elevated coagulation disorder score as a quartile variable was significantly associated with increased all-cause mortality (quartile 4 vs. quartile 1, 30-day: HR [95% CI], 1.98 [1.50, 2.62], 90-day: HR [95% CI], 1.88 [1.49, 2.37], in-hospital: HR [95%CI], 1.93 [1.42, 2.61]).
In critically ill patients with CHF, ones with high coagulation disorder score tend to be worse clinical prognosis, which would be a promising biomarker and helpful for the management of CHF patients.
充血性心力衰竭(CHF)中的凝血功能障碍已有充分记录。一种综合凝血功能障碍评分,该评分结合了血小板计数绝对值、国际标准化比值(INR)和活化部分凝血活酶时间(APTT),其预后价值在CHF中尚未得到评估。本研究旨在探讨凝血功能障碍评分与重症CHF患者不良结局之间的关联。
本回顾性队列研究纳入了重症监护医学信息数据库III(MIMIC-III)中诊断为CHF的患者。根据重症监护病房入院后24小时内血小板计数绝对值、INR和APTT的异常情况计算凝血功能障碍评分。主要结局是短期全因死亡率,包括30天、90天和住院死亡率。采用Kaplan-Meier(K-M)生存曲线和Cox比例风险模型评估凝血功能障碍评分与结局事件之间的相关性。
本研究共纳入6895例患者,并根据凝血功能障碍评分分为四组。K-M生存曲线初步表明,凝血功能障碍评分较高的受试者生存率较低,生存时间较短。在对潜在混杂因素进行调整后,多变量Cox分析进一步表明,作为四分位数变量的凝血功能障碍评分升高与全因死亡率增加显著相关(四分位数4与四分位数1相比,30天:HR[第95百分位区间],1.98[1.50,2.62],90天:HR[第95百分位区间],1.88[1.49,2.37],住院:HR[第95百分位区间],1.93[1.42,2.61])。
在重症CHF患者中,凝血功能障碍评分高的患者临床预后往往较差,这将是一个有前景的生物标志物,有助于CHF患者的管理。