Straeuli Christopher, Jenkins Louis, Droomer Nardus
George Regional Hospital, George, Garden Route District, Western Cape Department of Health.
Department of Family and Emergency Medicine, Faculty of Health Sciences, University of Stellenbosch, Cape Town, South Africa.
Afr J Emerg Med. 2022 Dec;12(4):387-392. doi: 10.1016/j.afjem.2022.08.006. Epub 2022 Sep 15.
: Globally, emergency centers (ECs) face increasing patients with palliative care (PC) needs. This is also true for South Africa. Factors include an increasingly older population, rising rates of non-communicable and infectious diseases. A paucity of data exists on local rates and reasons for patients with life limiting conditions presenting to ECs. PC and emergency medicine are established specialties, but little is known how they interface in clinical practice. This study describes the contribution of patients with life limiting conditions to the case load of an EC in a regional hospital in the Western Cape.
: This was a prospective, descriptive study. All patients entering the EC over 3 months were assessed using a validated PC identification tool, developed for low-and-middle-income countries. All patients entering the EC were captured in an electronic database. Those identified to have life limiting illnesses and potential PC needs received a secondary ICD-10 code. These files were extracted and statistically analysed. Variables included diagnosis, demographics, reason for visit, and disposition.
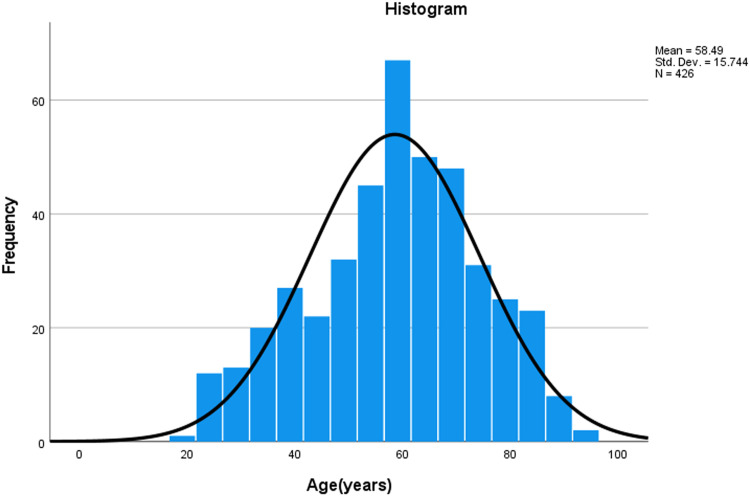
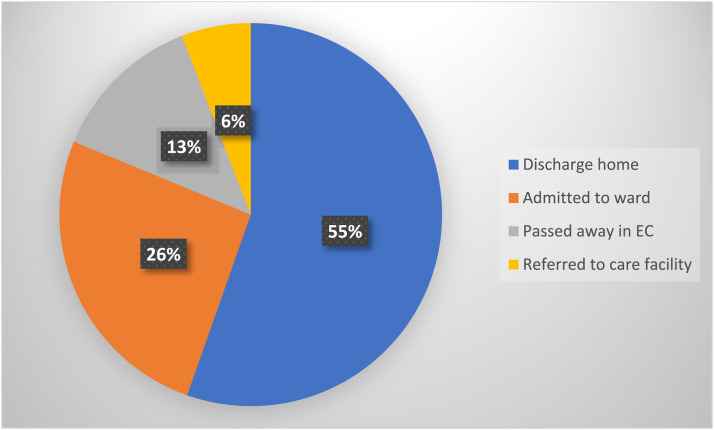
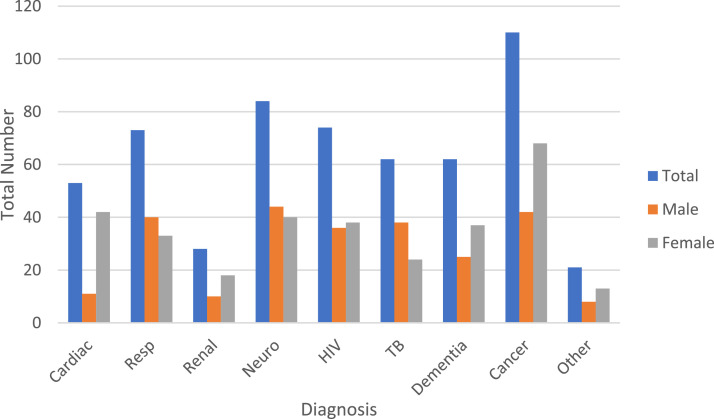
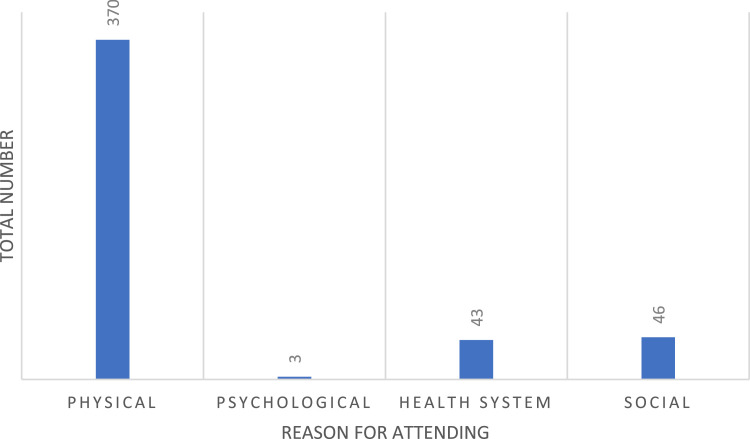
: A total of 426 patient visits (4.24%) were identified. Cancer (25.8%), neurological (19.7%) and HIV (17.4%) were the most frequent diagnoses. Patients with HIV and TB were significantly younger. Physical symptoms were the most common reasons for attendance (87%), followed by social (11%) and system issues (10%). Most patients were discharged home (55%), 26% were admitted, and 13% died in the EC.
: ECs in Africa are under-resourced and uncomfortable places for patients with life limiting illnesses. System-related visits could be avoidable, as most were due to patients running out of medication or requiring procedures such as urinary catheter changes, which could be done at the local clinic. Some attended EC due to social reasons, usually due to caregivers feeling overwhelmed. Patients requiring PC make up a significant percentage of EC visits. Optimizing health systems and community home-based care could alleviate EC pressures and improve the illness experience of patients with life limiting conditions.
在全球范围内,急诊中心(ECs)面临着越来越多有姑息治疗(PC)需求的患者。南非也是如此。影响因素包括人口老龄化加剧、非传染性疾病和传染病发病率上升。关于当地生命受限疾病患者前往急诊中心的比例和原因的数据匮乏。姑息治疗和急诊医学是既定的专业,但对于它们在临床实践中的衔接方式知之甚少。本研究描述了生命受限疾病患者对西开普省一家地区医院急诊中心病例量的贡献。
这是一项前瞻性描述性研究。使用为低收入和中等收入国家开发的经过验证的姑息治疗识别工具,对所有在3个月内进入急诊中心的患者进行评估。所有进入急诊中心的患者都被录入电子数据库。那些被确定患有生命受限疾病和潜在姑息治疗需求的患者被赋予二级国际疾病分类第十版(ICD - 10)编码。提取这些文件并进行统计分析。变量包括诊断、人口统计学特征、就诊原因和处置情况。
共识别出426例患者就诊(占4.24%)。癌症(25.8%)、神经系统疾病(19.7%)和艾滋病毒(17.4%)是最常见的诊断。感染艾滋病毒和结核病的患者明显更年轻。身体症状是就诊的最常见原因(87%),其次是社会原因(11%)和系统问题(10%)。大多数患者出院回家(55%),26%入院,13%在急诊中心死亡。
非洲的急诊中心资源不足,对于患有生命受限疾病的患者来说环境不佳。与系统相关的就诊情况本可避免,因为大多数是由于患者药物用完或需要进行诸如更换导尿管等操作,而这些操作可在当地诊所进行。一些患者因社会原因就诊,通常是由于护理人员不堪重负。需要姑息治疗的患者占急诊中心就诊患者的很大比例。优化卫生系统和社区居家护理可以减轻急诊中心的压力,并改善生命受限疾病患者的患病体验。