Department of Orthopedics and Traumatology, Medicine Faculty of Istinye University, İstanbul, Turkey.
Department of Orthopedics and Traumatology, Istinye University Training and Research Hospital, İstanbul, Turkey.
Medicine (Baltimore). 2022 Sep 23;101(38):e30823. doi: 10.1097/MD.0000000000030823.
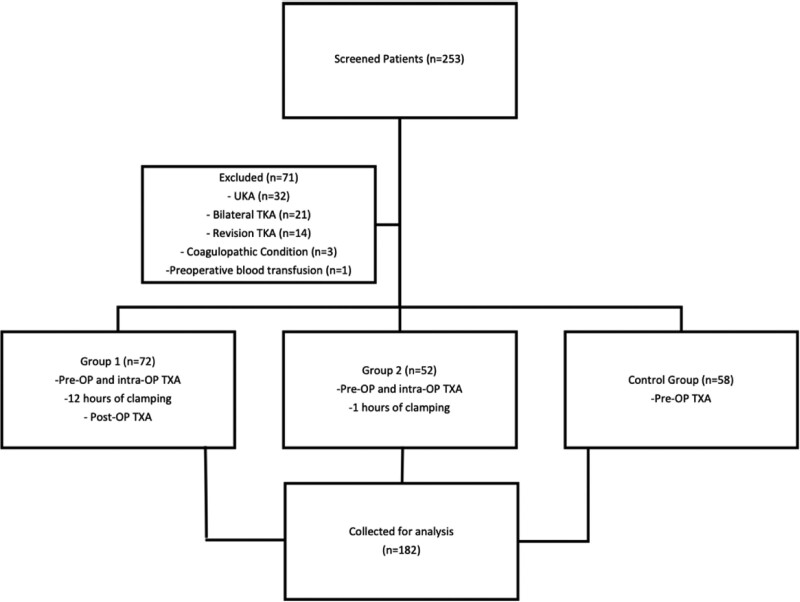
Many different methods and drain clamping periods have been described in systemic and local tranexamic acid (TXA) applications, and the superiority of the methods to each other has not been clearly demonstrated. The method of local infusion in combined TXA applications may not alter the Hb drop or total or hidden blood loss. We aim to compare two different combined TXA application methods. We retrospectively analyzed 182 patients who underwent total knee arthroplasty between 2018 and 2021. Patients over 40 years of age who underwent TKA for degenerative knee arthritis were included in the study. Unicondylar, revision, or bilateral arthroplasties and patients with the cardiovascular or cerebrovascular disease were excluded from the study. All patients in the study received 1 g TXA intravenously half an hour before the incision. For the first group, 1 g TXA was given intra-articularly at the drain site after closure, and the clamp was kept closed for 1 hour. In the second group, the drain was clamped for an additional 6 hours, and a 1 g intravenous dose was administered at the 5th hour postoperatively. No local applications were used in the control group. Total, hidden, and visible blood loss (total blood loss, hidden blood loss, visible blood loss), postoperative decreases in hemoglobin and hematocrit level (ΔHgb, ΔHtc), blood transfusion rates, and hospital stay durations were evaluated. There were 72 patients in the first group, 52 in the second, and 58 in control. A total of 37 patients received one or more blood transfusions postoperatively, and there was no statistical difference in the need for blood transfusions between the groups (P = .255). Although a statistically significant difference (P = .001) in total blood loss, hidden blood loss, visible blood loss and ΔHgb values was observed between the groups, the difference between the first and second groups was insignificant (P = .512). The duration of hospital stay was observed to be less in the first and second groups (P = .024). Local and systemic TXA applications were observed to be more effective than only systemic applications in reducing blood loss after total knee arthroplasty, regardless of the local method.
许多不同的方法和引流夹闭时间已在全身性和局部氨甲环酸(TXA)应用中被描述,且彼此之间哪种方法更优尚未明确。局部灌注联合 TXA 应用的方法可能不会改变 Hb 下降或总失血量或隐性失血量。我们旨在比较两种不同的联合 TXA 应用方法。我们回顾性分析了 2018 年至 2021 年间接受全膝关节置换术的 182 例患者。该研究纳入了年龄超过 40 岁、因退行性膝关节炎行 TKA 的患者。排除单髁、翻修或双侧关节置换术以及心血管或脑血管疾病患者。所有患者在术前半小时静脉给予 1gTXA。对于第 1 组,在关闭后于引流部位关节内给予 1gTXA,并保持夹闭 1 小时。在第 2 组中,引流管夹闭时间延长 6 小时,术后第 5 小时给予 1g 静脉剂量。对照组未局部应用。评估总失血量、隐性失血量、显性失血量(总失血量、隐性失血量、显性失血量)、术后血红蛋白和红细胞压积水平下降(ΔHgb、ΔHtc)、输血率和住院时间。第 1 组有 72 例患者,第 2 组有 52 例患者,对照组有 58 例患者。共有 37 例患者术后需要输血,各组间输血需求无统计学差异(P=0.255)。尽管组间总失血量、隐性失血量、显性失血量和ΔHgb 值存在统计学显著差异(P=0.001),但第 1 组和第 2 组之间的差异无统计学意义(P=0.512)。第 1 组和第 2 组的住院时间观察到较短(P=0.024)。局部和全身 TXA 应用比仅全身应用更有效,可减少全膝关节置换术后的失血,无论局部方法如何。