Lotan Itay, Nishiyama Shuhei, Manzano Giovanna S, Lydston Melissa, Levy Michael
Division of Neuroimmunology and Neuroinfectious Disease, Department of Neurology, Massachusetts General Hospital and Harvard Medical School, Boston, MA, United States.
Treadwell Virtual Library for the Massachusetts General Hospital, Boston, MA, United States.
Front Neurol. 2022 Sep 20;13:970383. doi: 10.3389/fneur.2022.970383. eCollection 2022.
Viral infections are a proposed possible cause of inflammatory central nervous system (CNS) demyelinating diseases, including multiple sclerosis (MS), neuromyelitis optica spectrum disorder (NMOSD), and myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD). During the past 2 years, CNS demyelinating events associated with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection have been reported, but causality is unclear.
To investigate the relationship between CNS demyelinating disease development and exacerbation with antecedent and/or concurrent SARS-CoV-2 infection.
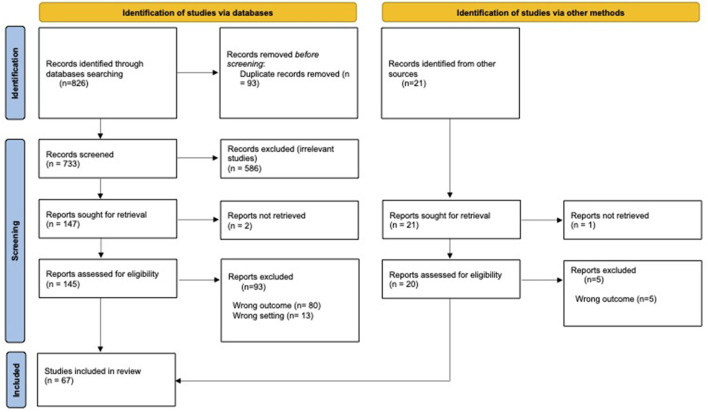
A systematic literature review of all publications describing either a new diagnosis or relapse of CNS demyelinating diseases (MS, NMOSD, MOGAD) in association with SARS-CoV-2 infection was performed utilizing PRISMA guidelines. Descriptive statistics were used for data analysis, using a case analysis approach.
Sixty-seven articles met the inclusion criteria for the study. Most of the reported cases of NMOSD ( = 13, 72.2% of reported cases) and MOGAD ( = 27, 96.5% of reported cases) were of new disease onset, presenting with typical clinical and radiographic features of these conditions, respectively. In contrast, reported MS cases varied amongst newly diagnosed cases ( = 10, 10.5% of reported cases), relapses ( = 63, 66.4%) and pseudo-relapses ( = 22, 23.2%). The median duration between COVID-19 infection and demyelinating event onset was 11.5 days (range 0-90 days) in NMOSD, 6 days (range-7 to +45 days) in MOGAD, and 13.5 days (range-21 to +180 days) in MS. Most cases received high-dose corticosteroids with a good clinical outcome.
Based upon available literature, the rate of CNS demyelinating events occurring in the setting of preceding or concurrent SARS-CoV-2 infection is relatively low considering the prevalence of SARS-CoV-2 infection. The clinical outcomes of new onset or relapsing MS, NMOSD, or MOGAD associated with antecedent or concurrent infection were mostly favorable. Larger prospective epidemiological studies are needed to better delineate the impact of COVID-19 on CNS demyelinating diseases.
病毒感染被认为是包括多发性硬化症(MS)、视神经脊髓炎谱系障碍(NMOSD)和髓鞘少突胶质细胞糖蛋白抗体相关疾病(MOGAD)在内的炎症性中枢神经系统(CNS)脱髓鞘疾病的一个可能病因。在过去两年中,已有与严重急性呼吸综合征冠状病毒2(SARS-CoV-2)感染相关的中枢神经系统脱髓鞘事件的报道,但因果关系尚不清楚。
探讨中枢神经系统脱髓鞘疾病的发生及加重与既往和/或同时发生的SARS-CoV-2感染之间的关系。
利用PRISMA指南对所有描述与SARS-CoV-2感染相关的中枢神经系统脱髓鞘疾病(MS、NMOSD、MOGAD)新诊断或复发的出版物进行系统的文献综述。采用病例分析方法进行描述性统计分析。
67篇文章符合该研究的纳入标准。大多数报告的NMOSD病例(13例,占报告病例的72.2%)和MOGAD病例(27例,占报告病例的96.5%)为新发病例,分别表现出这些疾病典型的临床和影像学特征。相比之下,报告的MS病例在新诊断病例(10例,占报告病例的10.5%)、复发病例(63例,占66.4%)和假性复发病例(22例,占23.2%)之间有所不同。在NMOSD中,COVID-19感染与脱髓鞘事件发作之间的中位持续时间为11.5天(范围0-90天),在MOGAD中为6天(范围-7至+45天),在MS中为13.5天(范围-21至+180天)。大多数病例接受了大剂量皮质类固醇治疗,临床结果良好。
根据现有文献,考虑到SARS-CoV-2感染的流行率,在既往或同时发生SARS-CoV-2感染的情况下发生中枢神经系统脱髓鞘事件的比率相对较低。与既往或同时感染相关的新发或复发MS、NMOSD或MOGAD的临床结果大多良好。需要开展更大规模的前瞻性流行病学研究,以更好地描述COVID-19对中枢神经系统脱髓鞘疾病的影响。