Usui Eisuke, Matsumura Mitsuaki, Smilowitz Nathaniel R, Mintz Gary S, Saw Jacqueline, Kwong Raymond Y, Hada Masahiro, Mahmud Ehtisham, Giesler Caitlin, Shah Binita, Bangalore Sripal, Razzouk Louai, Hoshino Masahiro, Marzo Kevin, Ali Ziad A, Bairey Merz C Noel, Sugiyama Tomoyo, Har Bryan, Kakuta Tsunekazu, Hochman Judith S, Reynolds Harmony R, Maehara Akiko
Clinical Trials Center, Cardiovascular Research Foundation, New York, NY 10019, USA.
Cardiovascular Research Foundation, New York-Presbyterian Hospital/Columbia University Irving Medical Center, 1700 Broadway, 9th Floor, New York, NY 10019, USA.
Eur Heart J Open. 2022 Sep 30;2(5):oeac058. doi: 10.1093/ehjopen/oeac058. eCollection 2022 Sep.
We aimed to use optical coherence tomography (OCT) to identify differences in atherosclerotic culprit lesion morphology in women with myocardial infarction (MI) with non-obstructive coronary arteries (MINOCA) compared with MI with obstructive coronary artery disease (MI-CAD).
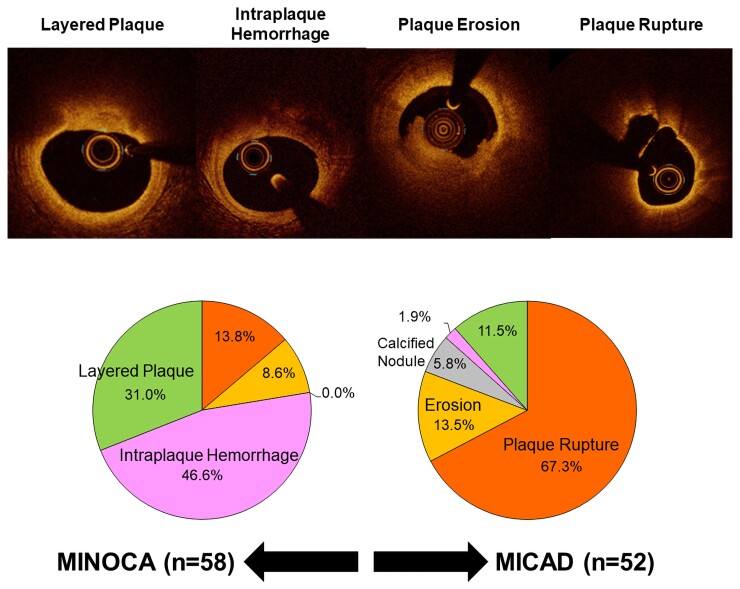
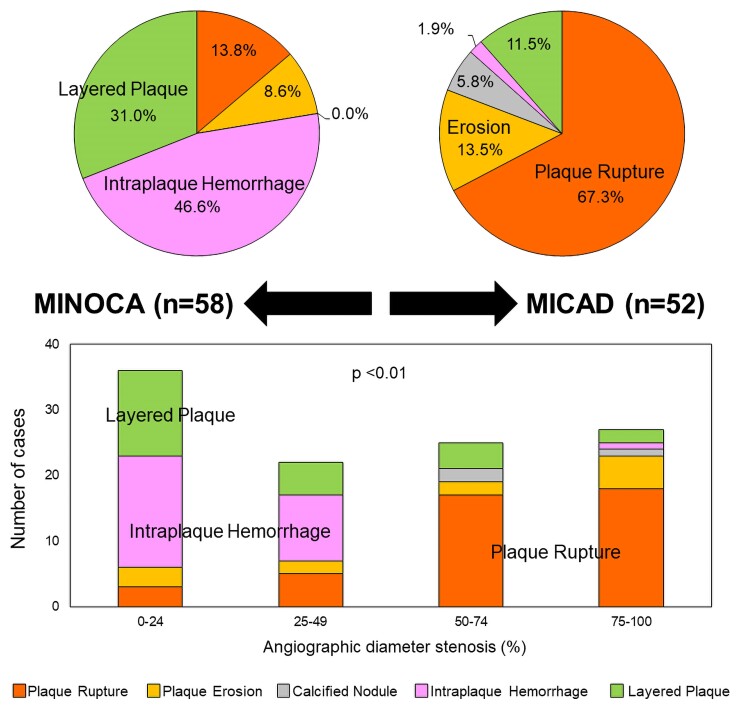
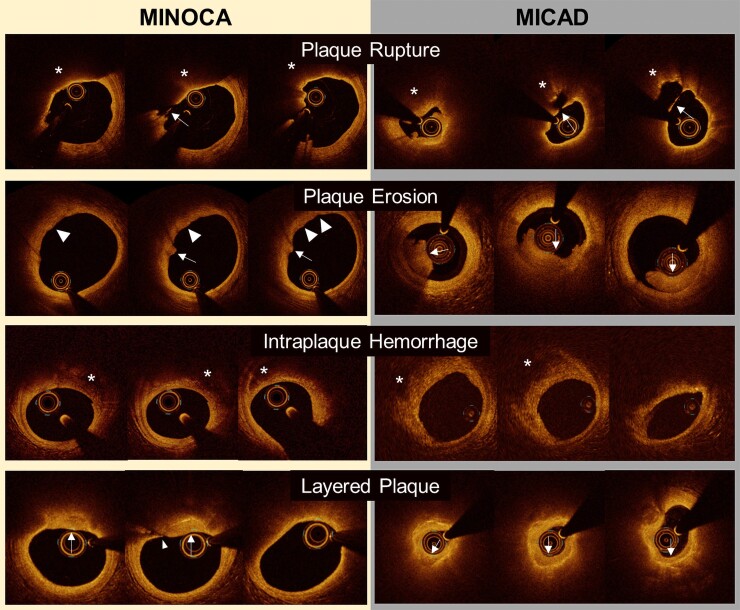
Women with an OCT-determined atherosclerotic aetiology of non-ST segment elevation (NSTE)-MINOCA (angiographic diameter stenosis <50%) who were enrolled in the multicentre Women's Heart Attack Research Program (HARP) study were compared with a consecutive series of women with NSTE-MI-CAD who underwent OCT prior to coronary intervention at a single institution. Atherosclerotic pathologies identified by OCT included plaque rupture, plaque erosion, intraplaque haemorrhage (IPH, a region of low signal intensity with minimum attenuation adjacent to a lipidic plaque without fibrous cap disruption), layered plaque (superficial layer with clear demarcation from the underlying plaque indicating early thrombus healing), or eruptive calcified nodule.We analysed 58 women with NSTE-MINOCA and 52 women with NSTE-MI-CAD. Optical coherence tomography features of underlying vulnerable plaque (thin-cap fibroatheroma) were less common in MINOCA (3 vs. 35%) than in MI-CAD. Intraplaque haemorrhage (47 vs. 2%) and layered plaque (31 vs. 12%) were more common in MINOCA than MI-CAD, whereas plaque rupture (14 vs. 67%), plaque erosion (8 vs. 14%), and calcified nodule (0 vs. 6%) were less common in MINOCA. The angle of ruptured cavity was smaller and thrombus burden was lower in MINOCA.
The prevalence of atherothrombotic culprit lesion subtype varied substantially between MINOCA and MI-CAD. A majority of culprit lesions in MINOCA had the appearance of IPH or layered plaque.
: Heart Attack Research Program- Imaging Study (HARP); : NCT02905357; : https://clinicaltrials.gov/ct2/show/NCT02905357.
我们旨在使用光学相干断层扫描(OCT)来确定非阻塞性冠状动脉心肌梗死(MINOCA)女性与阻塞性冠状动脉疾病心肌梗死(MI-CAD)女性的动脉粥样硬化罪犯病变形态差异。
将多中心女性心脏病发作研究项目(HARP)中纳入的、经OCT确定为非ST段抬高型(NSTE)-MINOCA(血管造影直径狭窄<50%)且病因是动脉粥样硬化的女性,与在单一机构接受冠状动脉介入治疗前接受OCT检查的一系列连续的NSTE-MI-CAD女性进行比较。OCT识别的动脉粥样硬化病变包括斑块破裂、斑块侵蚀、斑块内出血(IPH,脂质斑块附近无纤维帽破裂的低信号强度且最小衰减区域)、分层斑块(表层与下层斑块有清晰分界,提示血栓早期愈合)或破裂性钙化结节。我们分析了58例NSTE-MINOCA女性和52例NSTE-MI-CAD女性。MINOCA中潜在易损斑块(薄帽纤维粥样瘤)的光学相干断层扫描特征比MI-CAD中少见(3%对35%)。MINOCA中斑块内出血(47%对2%)和分层斑块(31%对12%)比MI-CAD中更常见,而MINOCA中斑块破裂(14%对67%)、斑块侵蚀(8%对14%)和钙化结节(0%对6%)则较少见。MINOCA中破裂腔的角度较小且血栓负荷较低。
MINOCA和MI-CAD之间动脉粥样硬化血栓形成罪犯病变亚型的患病率差异很大。MINOCA中的大多数罪犯病变表现为IPH或分层斑块。
心脏病发作研究项目-成像研究(HARP);NCT02905357;https://clinicaltrials.gov/ct2/show/NCT02905357 。