Rios Olina, Lerhe Barbara, Chamorey Emmanuel, Savoldelli Charles
Department of Oral and Maxillo-Facial Surgery, Head and Neck Institute, 06100 Nice, France.
Department of Statistics, Antoine Lacassagne Center, 06100 Nice, France.
J Clin Med. 2022 Sep 20;11(19):5495. doi: 10.3390/jcm11195495.
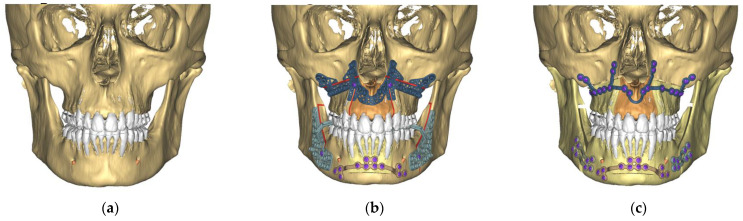
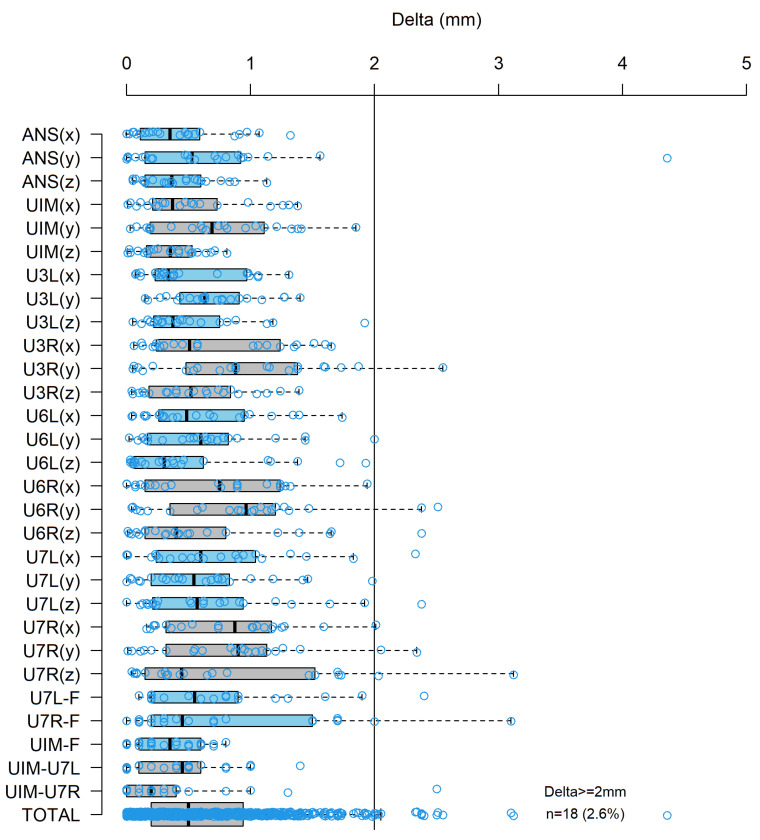
Background: When maxillary transversal expansion is needed, two protocols of treatment can be used: a maxillary orthodontic expansion followed by a classical bimaxillary osteotomy or a bimaxillary osteotomy with maxillary segmentation. The aim of this study was to assess the accuracy of segmented Le Fort I osteotomy using computer-aided orthognathic surgery and patient-specific titanium plates in patients who underwent a bimaxillary osteotomy for occlusal trouble with maxillary transversal insufficiencies. Methods: A virtual simulation of a Le Fort I osteotomy with maxillary segmentation, a sagittal split ramus osteotomy, and genioplasty (if needed) was conducted on a preoperative three-dimensional (3D) model of each patient’s skull using ProPlan CMF 3.0 software (Materialise, Leuven, Belgium). Computer-assisted osteotomy saw-and-drill guides and patient-specific implants (PSIs, titanium plates) were produced and used during the surgery. We chose to focus on the maxillary repositioning accuracy by comparing the preoperative virtual surgical planning and the postoperative 3D outcome skulls using surface superimpositions and 13 standard dental and bone landmarks. Errors between these preoperative and postoperative landmarks were calculated and compared to discover if segmental maxillary repositioning using PSIs was accurate enough to be safely used to treat transversal insufficiencies. Results: A total of 22 consecutive patients—15 females and 7 males, with a mean age of 27.4 years—who underwent bimaxillary computer-assisted orthognathic surgery with maxillary segmentation were enrolled in the study. All patients presented with occlusion trouble, 13 with Class III malocclusions (59%) and 9 (41%) with Class II malocclusions. A quantitative analysis revealed that, overall, the mean absolute discrepancies for the x-axis (transversal dimension), y-axis (anterior−posterior dimensions), and z-axis (vertical dimension) were 0.59 mm, 0.74 mm, and 0.56 mm, respectively. The total error rate of maxillary repositioning was 0.62 mm between the postoperative cone-beam computed tomography (CBCT) and the preoperatively planned 3D skull. According to the literature, precision in maxilla repositioning is defined by an error rate (clinically relevant) at each landmark of <2 mm and a total error of <2 mm for each patient. Conclusions: A high degree of accuracy between the virtual plan and the postoperative result was observed.
当需要进行上颌横向扩展时,可采用两种治疗方案:先进行上颌正畸扩展,然后进行经典的双颌截骨术,或进行上颌分段的双颌截骨术。本研究的目的是评估在因上颌横向发育不足导致咬合问题而接受双颌截骨术的患者中,使用计算机辅助正颌手术和患者特异性钛板进行分段Le Fort I截骨术的准确性。方法:使用ProPlan CMF 3.0软件(Materialise,比利时鲁汶)对每位患者术前的颅骨三维(3D)模型进行Le Fort I上颌分段截骨术、下颌升支矢状劈开截骨术和颏成形术(如有需要)的虚拟模拟。手术过程中制作并使用了计算机辅助截骨锯和钻头导向器以及患者特异性植入物(PSI,钛板)。我们选择通过使用表面叠加和13个标准牙齿及骨标志点比较术前虚拟手术规划和术后3D颅骨结果,来关注上颌重新定位的准确性。计算并比较这些术前和术后标志点之间的误差,以发现使用PSI进行上颌分段重新定位是否足够准确,可安全用于治疗横向发育不足。结果:本研究共纳入22例连续接受上颌分段的双颌计算机辅助正颌手术的患者,其中女性15例,男性7例,平均年龄27.4岁。所有患者均存在咬合问题,13例为III类错牙合(59%),9例(41%)为II类错牙合。定量分析显示,总体而言,x轴(横向维度)、y轴(前后维度)和z轴(垂直维度)的平均绝对差异分别为0.59 mm、0.74 mm和0.56 mm。术后锥形束计算机断层扫描(CBCT)与术前规划的3D颅骨之间上颌重新定位的总误差率为0.62 mm。根据文献,上颌重新定位的精度定义为每个标志点的误差率(临床相关)<2 mm,每位患者的总误差<2 mm。结论:观察到虚拟计划与术后结果之间具有高度准确性。