Médecine Intensive Réanimation, Hôpital de Hautepierre, Hôpitaux Universitaires de Strasbourg, Fédération de Médecine Translationnelle de Strasbourg (FMTS) and Unistra, Strasbourg, France.
Institut National de la Santé et de la Recherche Médicale-Unité Mixte de Recherche (INSERM-UMR) 1121 Biomatériaux et Bio-ingénierie, Fédération de Médecine Translationnelle de Strasbourg (FMTS) and Unistra, Strasbourg, France.
Front Immunol. 2022 Sep 29;13:985472. doi: 10.3389/fimmu.2022.985472. eCollection 2022.
Neuroendocrine cells release Catestatin (CST) from Chromogranin A (CgA) to regulate stress responses. As regards COVID-19 patients (COVID+) requiring oxygen supply, to date nobody has studied CST as a potential mediator in the regulation of immunity.
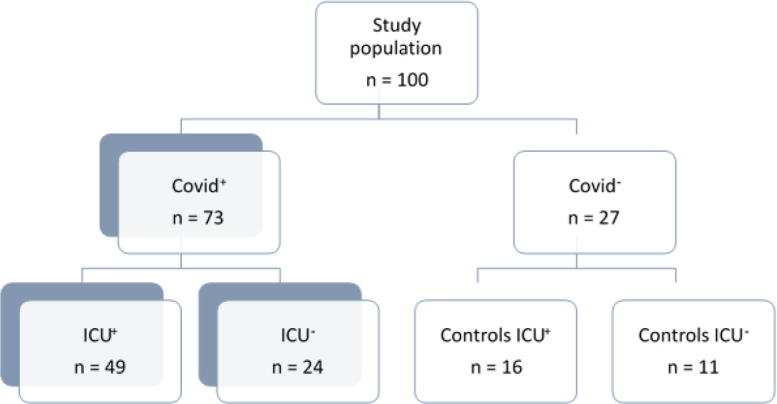
PATIENTS & METHODS: Admission plasma CST and CgA - its precursor - concentrations were measured (ELISA test) in 73 COVID+ and 27 controls. Relationships with demographics, comorbidities, disease severity and outcomes were analysed (Mann-Whitney, Spearman correlation tests, ROC curves).
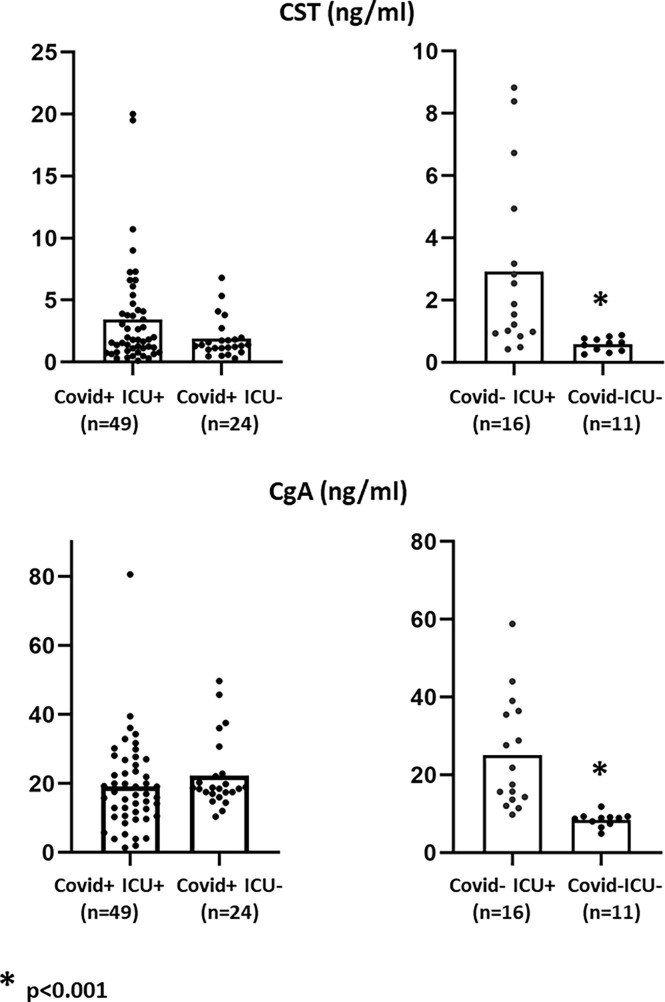
Among COVID+, 49 required ICU-admission (COVID+ICU+) and 24 standard hospitalization (COVID+ICU-). Controls were either healthy staff (COVID-ICU-, n=11) or COVID-ICU+ patients (n=16). Median plasma CST were higher in COVID+ than in controls (1.6 [1.02; 3.79] 0.87 [0.59; 2.21] ng/mL, <0.03), with no difference between COVID+ and COVID-ICU+. There was no difference between groups in either CgA or CST/CgA ratios, but these parameters were lower in healthy controls (<0.01). CST did not correlate with either hypoxia- or usual inflammation-related parameters. In-hospital mortality was similar whether COVID+ or not, but COVID+ had longer oxygen support and more complications (<0.03). CST concentrations and the CST/CgA ratio were associated with in-hospital mortality (<0.01) in COVID+, whereas CgA was not. CgA correlated with care-related infections (<0.001).
Respiratory COVID patients release significant amounts of CST in the plasma making this protein widely available for the neural regulation of immunity. If confirmed prospectively, plasma CST will reliably help in predicting in-hospital mortality, whereas CgA will facilitate the detection of patients prone to care-related infections.
神经内分泌细胞从嗜铬粒蛋白 A (CgA) 中释放 Catestatin (CST) 以调节应激反应。关于需要供氧的 COVID-19 患者 (COVID+),迄今为止,没有人研究 CST 作为调节免疫的潜在介质。
测量了 73 例 COVID+ 和 27 例对照者入院时的血浆 CST 和 CgA(其前体)浓度(ELISA 试验)。分析了与人口统计学、合并症、疾病严重程度和结局的关系(Mann-Whitney、Spearman 相关检验、ROC 曲线)。
在 COVID+中,49 例需要 ICU 入院 (COVID+ICU+),24 例标准住院 (COVID+ICU-)。对照组为健康工作人员 (COVID-ICU-,n=11) 或 COVID+ICU+患者 (n=16)。COVID+患者的血浆 CST 中位数高于对照组 (1.6 [1.02; 3.79] vs. 0.87 [0.59; 2.21] ng/mL,<0.03),COVID+和 COVID-ICU+之间无差异。CgA 或 CST/CgA 比值在各组之间无差异,但健康对照组较低 (<0.01)。CST 与缺氧或常规炎症相关参数均无相关性。无论 COVID+与否,住院死亡率相似,但 COVID+的氧疗时间更长,并发症更多(<0.03)。CST 浓度和 CST/CgA 比值与 COVID+患者的住院死亡率相关 (<0.01),而 CgA 则不然。CgA 与与护理相关的感染相关 (<0.001)。
COVID 患者的呼吸道释放大量 CST 进入血浆,使这种蛋白广泛用于神经调节免疫。如果前瞻性得到证实,血浆 CST 将可靠地帮助预测住院死亡率,而 CgA 将有助于发现易发生与护理相关的感染的患者。