Deng Yuhan, Liu Shuang, Wang Ziyao, Wang Yuxin, Jiang Yong, Liu Baohua
School of Public Health, Peking University, Beijing, China.
Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China.
Front Med (Lausanne). 2022 Sep 28;9:933037. doi: 10.3389/fmed.2022.933037. eCollection 2022.
In-hospital mortality, prolonged length of stay (LOS), and 30-day readmission are common outcomes in the intensive care unit (ICU). Traditional scoring systems and machine learning models for predicting these outcomes usually ignore the characteristics of ICU data, which are time-series forms. We aimed to use time-series deep learning models with the selective combination of three widely used scoring systems to predict these outcomes.
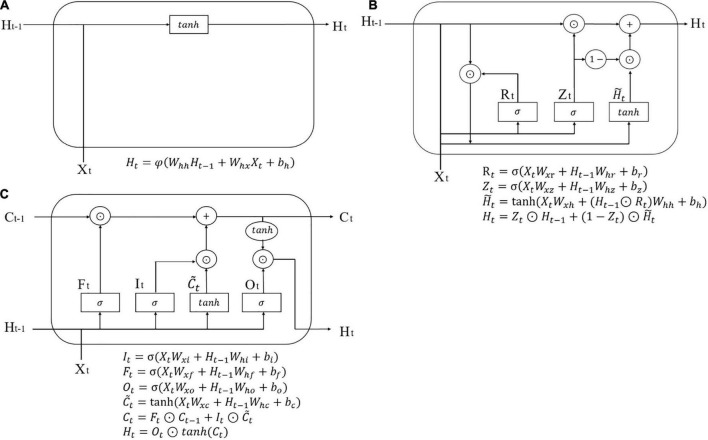
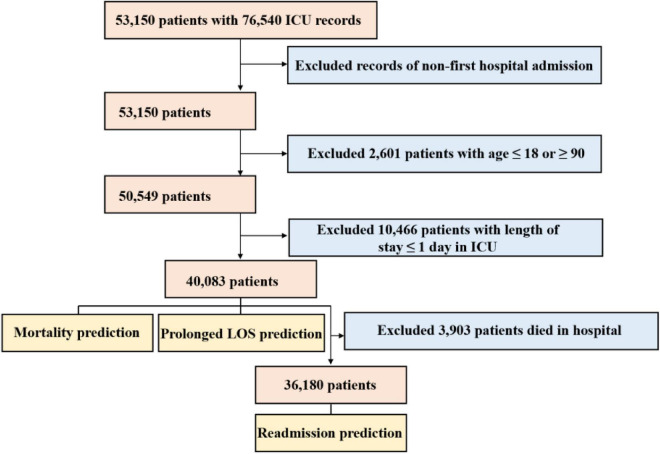
A retrospective cohort study was conducted on 40,083 patients in ICU from the Medical Information Mart for Intensive Care-IV (MIMIC-IV) database. Three deep learning models, namely, recurrent neural network (RNN), gated recurrent unit (GRU), and long short-term memory (LSTM) with attention mechanisms, were trained for the prediction of in-hospital mortality, prolonged LOS, and 30-day readmission with variables collected during the initial 24 h after ICU admission or the last 24 h before discharge. The inclusion of variables was based on three widely used scoring systems, namely, APACHE II, SOFA, and SAPS II, and the predictors consisted of time-series vital signs, laboratory tests, medication, and procedures. The patients were randomly divided into a training set (80%) and a test set (20%), which were used for model development and model evaluation, respectively. The area under the receiver operating characteristic curve (AUC), sensitivity, specificity, and Brier scores were used to evaluate model performance. Variable significance was identified through attention mechanisms.
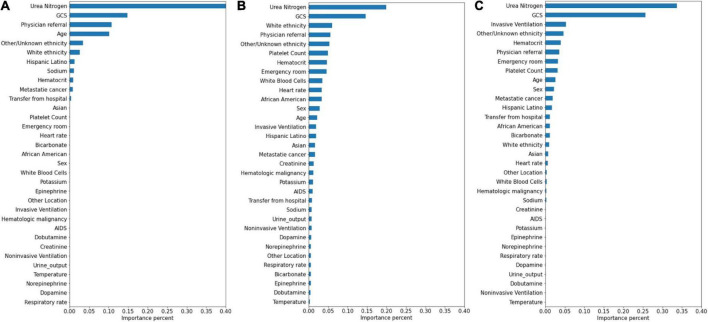
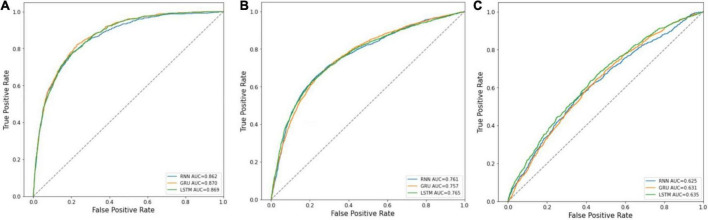
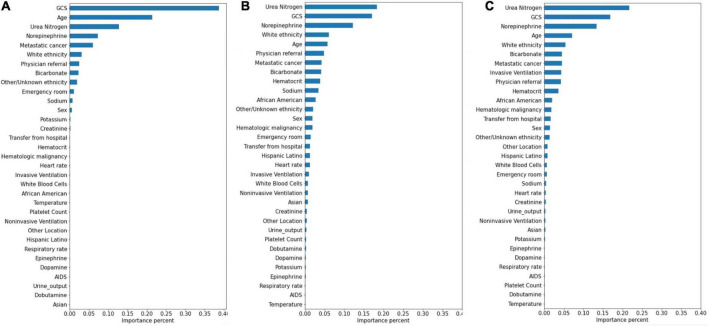
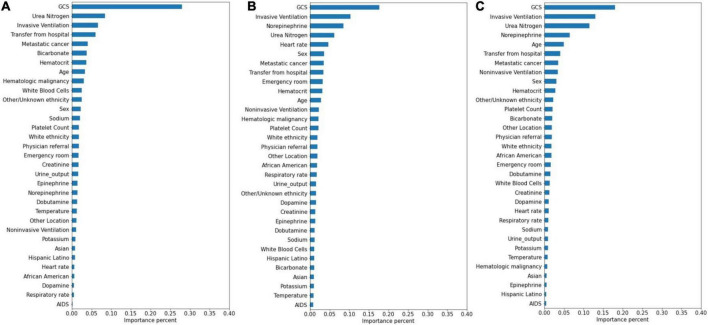
A total of 33 variables for 40,083 patients were enrolled for mortality and prolonged LOS prediction and 36,180 for readmission prediction. The rates of occurrence of the three outcomes were 9.74%, 27.54%, and 11.79%, respectively. In each of the three outcomes, the performance of RNN, GRU, and LSTM did not differ greatly. Mortality prediction models, prolonged LOS prediction models, and readmission prediction models achieved AUCs of 0.870 ± 0.001, 0.765 ± 0.003, and 0.635 ± 0.018, respectively. The top significant variables co-selected by the three deep learning models were Glasgow Coma Scale (GCS), age, blood urea nitrogen, and norepinephrine for mortality; GCS, invasive ventilation, and blood urea nitrogen for prolonged LOS; and blood urea nitrogen, GCS, and ethnicity for readmission.
The prognostic prediction models established in our study achieved good performance in predicting common outcomes of patients in ICU, especially in mortality prediction. In addition, GCS and blood urea nitrogen were identified as the most important factors strongly associated with adverse ICU events.
院内死亡率、住院时间延长(LOS)和30天再入院是重症监护病房(ICU)常见的结局。用于预测这些结局的传统评分系统和机器学习模型通常忽略了ICU数据的特征,这些数据是时间序列形式的。我们旨在使用时间序列深度学习模型,并选择性地结合三种广泛使用的评分系统来预测这些结局。
对医学重症监护信息数据库-IV(MIMIC-IV)中40,083例ICU患者进行回顾性队列研究。训练了三种深度学习模型,即具有注意力机制的递归神经网络(RNN)、门控递归单元(GRU)和长短期记忆(LSTM),以预测ICU入院后最初24小时或出院前最后24小时收集的变量的院内死亡率、住院时间延长和30天再入院情况。变量的纳入基于三种广泛使用的评分系统,即急性生理与慢性健康状况评分系统II(APACHE II)、序贯器官衰竭评估(SOFA)和简化急性生理学评分系统II(SAPS II),预测因素包括时间序列生命体征、实验室检查、用药和操作。患者被随机分为训练集(80%)和测试集(20%),分别用于模型开发和模型评估。采用受试者操作特征曲线下面积(AUC)、敏感性、特异性和布里尔评分来评估模型性能。通过注意力机制确定变量的重要性。
共纳入40,083例患者的33个变量用于死亡率和住院时间延长预测,36,180个变量用于再入院预测。三种结局的发生率分别为9.74%、27.54%和11.79%。在三种结局中,RNN、GRU和LSTM的性能差异不大。死亡率预测模型、住院时间延长预测模型和再入院预测模型的AUC分别为0.870±0.001、0.765±0.003和0.635±0.018。三种深度学习模型共同选择的最重要变量为:死亡率方面,格拉斯哥昏迷量表(GCS)、年龄、血尿素氮和去甲肾上腺素;住院时间延长方面,GCS、有创通气和血尿素氮;再入院方面,血尿素氮、GCS和种族。
我们研究中建立的预后预测模型在预测ICU患者常见结局方面表现良好,尤其是在死亡率预测方面。此外,GCS和血尿素氮被确定为与不良ICU事件密切相关的最重要因素。