Instituto de Investigación Biosanitaria ibs.GRANADA, Granada, Spain.
Escuela Andaluza de Salud Pública (EASP), Granada, Spain.
PLoS Med. 2022 Oct 20;19(10):e1004110. doi: 10.1371/journal.pmed.1004110. eCollection 2022 Oct.
Longer time intervals to diagnosis and treatment are associated with worse survival for various types of cancer. The patient, diagnostic, and treatment intervals are considered core indicators for early diagnosis and treatment. This review estimated the median duration of these intervals for various types of cancer and compared it across high- and lower-income countries.
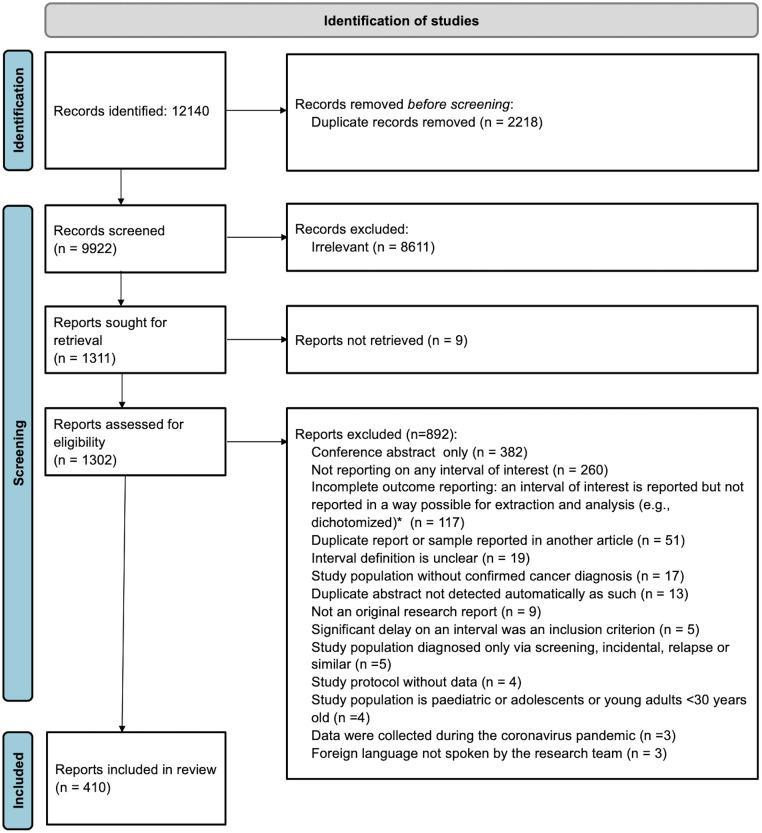
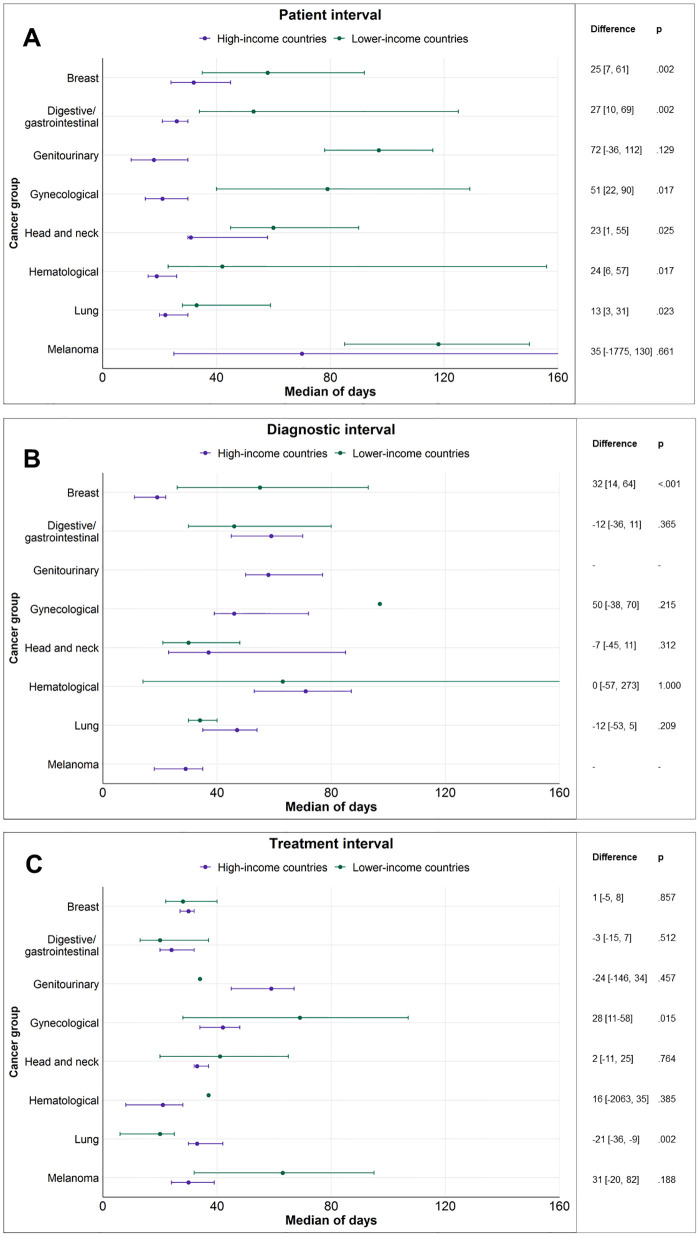
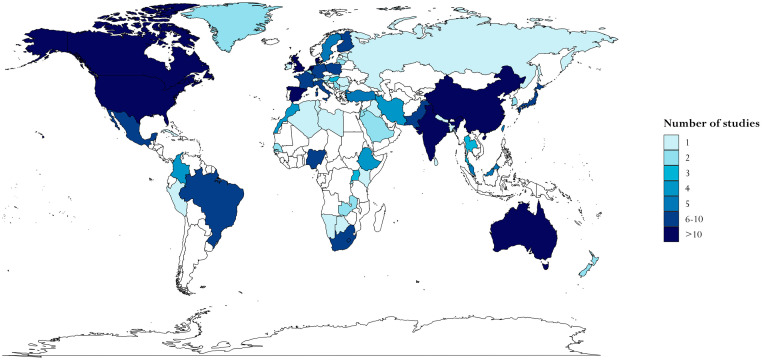
We conducted a systematic review with meta-analysis (prospectively registered protocol CRD42020200752). Three databases (MEDLINE, Embase, and Web of Science) and information sources including grey literature (Google Scholar, OpenGrey, EThOS, ProQuest Dissertations & Theses) were searched. Eligible articles were published during 2009 to 2022 and reported the duration of the following intervals in adult patients diagnosed with primary symptomatic cancer: patient interval (from the onset of symptoms to first presentation to a healthcare professional), diagnostic interval (from first presentation to diagnosis), and treatment interval (from diagnosis to treatment start). Interval duration was recorded in days and study medians were combined in a pooled estimate with 95% confidence intervals (CIs). The methodological quality of studies was assessed using the Aarhus checklist. A total of 410 articles representing 68 countries and reporting on 5,537,594 patients were included. The majority of articles reported data from high-income countries (n = 294, 72%), with 116 (28%) reporting data from lower-income countries. Pooled meta-analytic estimates were possible for 38 types of cancer. The majority of studies were conducted on patients with breast, lung, colorectal, and head and neck cancer. In studies from high-income countries, pooled median patient intervals generally did not exceed a month for most cancers. However, in studies from lower-income countries, patient intervals were consistently 1.5 to 4 times longer for almost all cancer sites. The majority of data on the diagnostic and treatment intervals came from high-income countries. Across both high- and lower-income countries, the longest diagnostic intervals were observed for hematological (71 days [95% CI 52 to 85], e.g., myelomas (83 days [47 to 145])), genitourinary (58 days [50 to 77], e.g., prostate (85 days [57 to 112])), and digestive/gastrointestinal (57 days [45 to 67], e.g., colorectal (63 days [48 to 78])) cancers. Similarly, the longest treatment intervals were observed for genitourinary (57 days [45 to 66], e.g., prostate (75 days [61 to 87])) and gynecological (46 days [38 to 54], e.g., cervical (69 days [45 to 108]) cancers. In studies from high-income countries, the implementation of cancer-directed policies was associated with shorter patient and diagnostic intervals for several cancers. This review included a large number of studies conducted worldwide but is limited by survivor bias and the inherent complexity and many possible biases in the measurement of time points and intervals in the cancer treatment pathway. In addition, the subintervals that compose the diagnostic interval (e.g., primary care interval, referral to diagnosis interval) were not considered.
These results identify the cancers where diagnosis and treatment initiation may take the longest and reveal the extent of global disparities in early diagnosis and treatment. Efforts should be made to reduce help-seeking times for cancer symptoms in lower-income countries. Estimates for the diagnostic and treatment intervals came mostly from high-income countries that have powerful health information systems in place to record such information.
对于各种类型的癌症,诊断和治疗之间的时间间隔越长,生存情况越差。患者、诊断和治疗间隔时间被认为是早期诊断和治疗的核心指标。本综述评估了各种类型癌症的这些间隔时间的中位数,并比较了高收入和低收入国家之间的差异。
我们进行了一项系统评价和荟萃分析(前瞻性注册方案 CRD42020200752)。我们检索了三个数据库(MEDLINE、Embase 和 Web of Science)和包括灰色文献(Google Scholar、OpenGrey、EThOS、ProQuest Dissertations & Theses)在内的信息源。合格的文章发表于 2009 年至 2022 年,报告了在成年原发性有症状癌症患者中以下间隔时间的持续时间:患者间隔(从症状出现到首次就诊于医疗保健专业人员)、诊断间隔(从首次就诊到诊断)和治疗间隔(从诊断到治疗开始)。间隔时间以天为单位记录,研究中位数采用 95%置信区间(CI)进行汇总估计。使用奥胡斯清单评估研究的方法学质量。共纳入 410 篇文章,代表 68 个国家,报告了 5537594 名患者的数据。大多数文章来自高收入国家(n=294,72%),116 篇(28%)来自低收入国家。对于 38 种癌症,可以进行汇总的meta 分析估计。大多数研究针对的是患有乳腺癌、肺癌、结直肠癌和头颈部癌症的患者。在来自高收入国家的研究中,大多数癌症的患者间隔时间一般不超过一个月。然而,在来自低收入国家的研究中,几乎所有癌症部位的患者间隔时间都持续长 1.5 至 4 倍。关于诊断和治疗间隔的大多数数据来自高收入国家。在高收入和低收入国家中,最长的诊断间隔时间见于血液系统(71 天[95%CI 52 至 85],例如骨髓瘤(83 天[47 至 145])、泌尿生殖系统(58 天[50 至 77],例如前列腺(85 天[57 至 112])和消化/胃肠道(57 天[45 至 67],例如结直肠癌(63 天[48 至 78]))癌症。同样,最长的治疗间隔时间见于泌尿生殖系统(57 天[45 至 66],例如前列腺(75 天[61 至 87])和妇科(46 天[38 至 54],例如宫颈癌(69 天[45 至 108])癌症。在来自高收入国家的研究中,癌症导向政策的实施与几种癌症的患者和诊断间隔时间缩短有关。本综述纳入了全球范围内的大量研究,但受到幸存者偏差以及癌症治疗途径中时间点和间隔测量固有的复杂性和多种可能偏差的限制。此外,未考虑组成诊断间隔的亚间隔(例如,初级保健间隔、转诊至诊断间隔)。
这些结果确定了诊断和治疗开始可能需要最长时间的癌症,并揭示了全球早期诊断和治疗方面的差异程度。应努力减少低收入国家癌症症状的求助时间。诊断和治疗间隔的估计值主要来自高收入国家,这些国家有强大的卫生信息系统来记录此类信息。