Peking University Peoples Hospital, Peking University Institute of Hematology, Beijing, 100044, P. R. China.
National Clinical Research Center for Hematologic Disease, Beijing, 100044, P. R. China.
Cancer Commun (Lond). 2022 Dec;42(12):1387-1402. doi: 10.1002/cac2.12376. Epub 2022 Oct 23.
Patients with refractory or relapsed acute myeloid leukemia (AML) have poor survival, necessitating the exploration of optimized therapeutic strategy. Here, we aimed to investigate clinical outcomes and health-related quality of life (HR-QoL) after total therapy, which included allogeneic hematopoietic stem cell transplantation (allo-HSCT), and prophylactic donor lymphocyte infusion (DLI) in the early phase after transplantation, followed by multiple measurable residual disease (MRD) and graft-versus-host disease (GvHD)-guided DLIs.
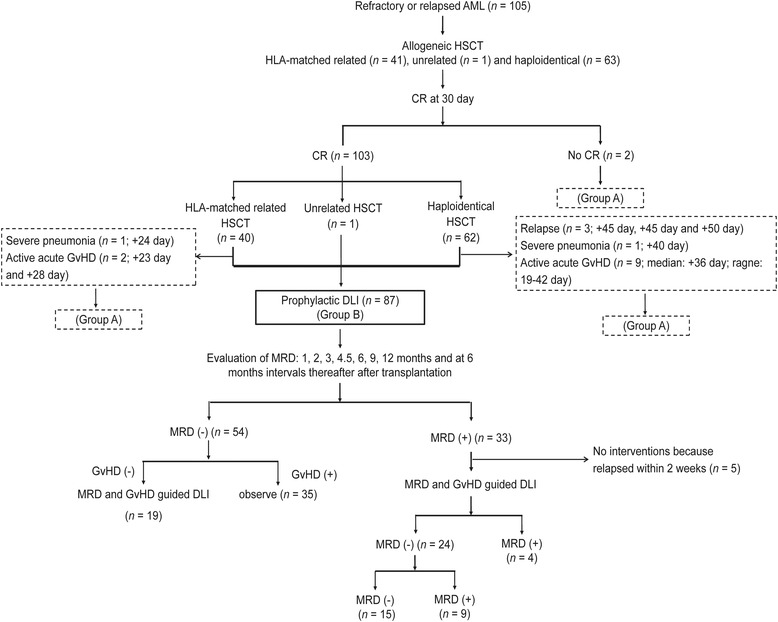
Consecutive patients who had refractory or relapsed AML and had received non-T-cell-depleted allo-HSCT at Peking University Institute of Hematology were included in the study. If the patients achieved complete remission at 30 days after transplantation and had no evidence of relapse, severe infection, organ failure, and active GvHD at the time of planned DLI, prophylactic DLI was administered at 30 days after transplantation for human leukocyte antigen (HLA)-matched related HSCT or at 45-60 days after transplantation for haploidentical or unrelated HSCT. Subsequently, multiple DLIs were administered based on MRD results and whether they developed GvHD after transplantation.
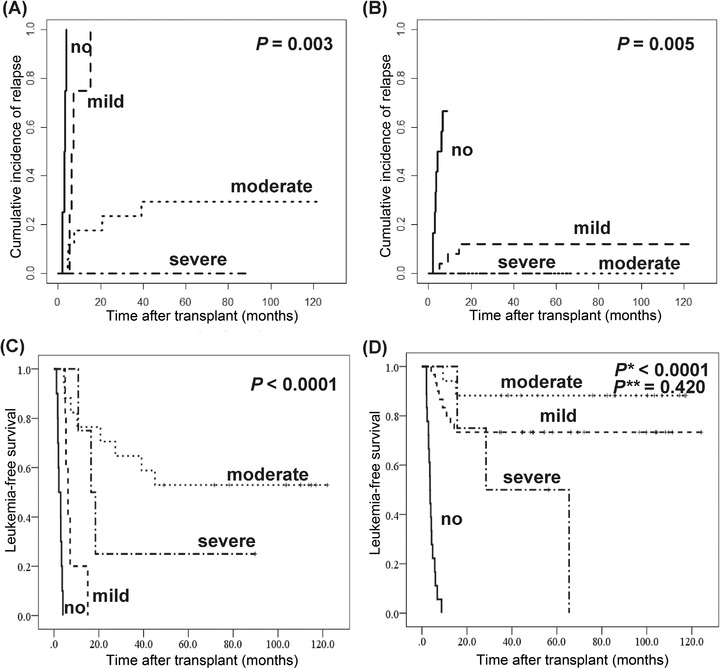
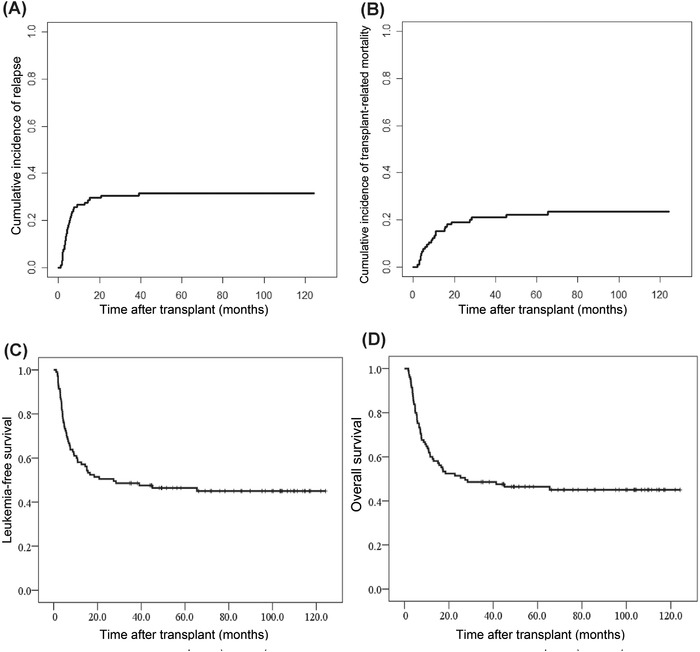
A total of 105 patients were eligible. Eighty-seven patients received prophylactic DLI (group B), while 18 did not receive prophylactic DLI (group A). Among 105 patients, the cumulative incidence of grade 2-4 acute GvHD and chronic GvHD was 40.6% (95% confidence interval [CI] = 30.6%-50.6%) and 73.3% (95% CI = 67.4%-79.2%), respectively. The cumulative incidence of relapse (CIR), transplant-related mortality (TRM), and leukemia-free survival (LFS) at 5 years after transplantation were 31.5% (95% CI = 21.9%-41.1%), 22.1% (95% CI = 11.3%-32.9%), and 46.4% (95% CI = 36.8%-56.0%), respectively. In group B, the CIR, TRM, and LFS at 5 years after transplantation were 27.6% (95% CI = 17.6%-37.6%), 21.6% (95% CI = 11.2%-32.0%), and 50.8% (95% CI = 40.0%-61.6%), respectively. At the end of follow-up, 48 patients survived, and more than 90% of survivors had satisfactory recoveries of HR-QoL.
Our study indicated that total therapy is not only associated with decreased CIR, comparable TRM, and better long-term LFS, but also with satisfactory HR-QoL for refractory or relapsed AML, compared with those of standard of care therapy reported previously. Therefore, total therapy may be an optimized therapeutic strategy for refractory or relapsed AML.
患有难治性或复发性急性髓系白血病(AML)的患者生存状况较差,需要探索优化的治疗策略。在这里,我们旨在研究在总治疗后(包括异基因造血干细胞移植(allo-HSCT)和移植后早期预防性供者淋巴细胞输注(DLI))的临床结局和与健康相关的生活质量(HR-QoL),随后根据多个可测量残留疾病(MRD)和移植物抗宿主病(GvHD)指导进行 DLI。
连续纳入在北京大学生物系接受非 T 细胞耗竭 allo-HSCT 的难治性或复发性 AML 患者。如果患者在移植后 30 天达到完全缓解,并且在计划进行 DLI 时没有复发、严重感染、器官衰竭和活动性 GvHD 的证据,则在移植后 30 天为 HLA 匹配的相关 HSCT 或移植后 45-60 天为单倍体或无关 HSCT 进行预防性 DLI。随后,根据 MRD 结果和移植后是否发生 GvHD 进行多次 DLI。
共有 105 名患者符合条件。87 名患者接受了预防性 DLI(B 组),而 18 名患者未接受预防性 DLI(A 组)。在 105 名患者中,2-4 级急性 GvHD 和慢性 GvHD 的累积发生率分别为 40.6%(95%CI=30.6%-50.6%)和 73.3%(95%CI=67.4%-79.2%)。移植后 5 年的复发累积发生率(CIR)、移植相关死亡率(TRM)和无白血病生存率(LFS)分别为 31.5%(95%CI=21.9%-41.1%)、22.1%(95%CI=11.3%-32.9%)和 46.4%(95%CI=36.8%-56.0%)。在 B 组中,移植后 5 年的 CIR、TRM 和 LFS 分别为 27.6%(95%CI=17.6%-37.6%)、21.6%(95%CI=11.2%-32.0%)和 50.8%(95%CI=40.0%-61.6%)。随访结束时,48 名患者存活,超过 90%的幸存者 HR-QoL 恢复良好。
与先前报道的标准治疗相比,我们的研究表明,总治疗不仅与降低 CIR、可比的 TRM 和更好的长期 LFS 相关,而且与难治性或复发性 AML 的可接受的 HR-QoL 相关。因此,总治疗可能是难治性或复发性 AML 的一种优化治疗策略。