Department of Anaesthesiology and Critical Care Medicine, University Medical Centre Mannheim, Medical Faculty Mannheim of the University of Heidelberg, Theodor-Kutzer Ufer 1-3, 68165, Mannheim, Germany.
Department of Cardiothoracic Anaesthesia and Intensive Care, Royal Papworth Hospital NHS Foundation Trust, Papworth Road, Cambridge Biomedical Campus, Cambridge, CB2 0AY, UK.
J Clin Monit Comput. 2023 Apr;37(2):599-607. doi: 10.1007/s10877-022-00931-0. Epub 2022 Oct 25.
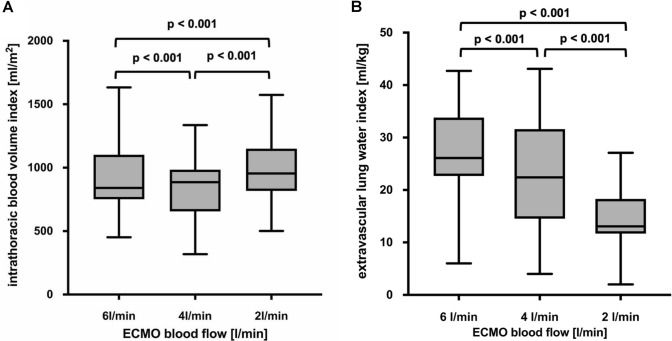
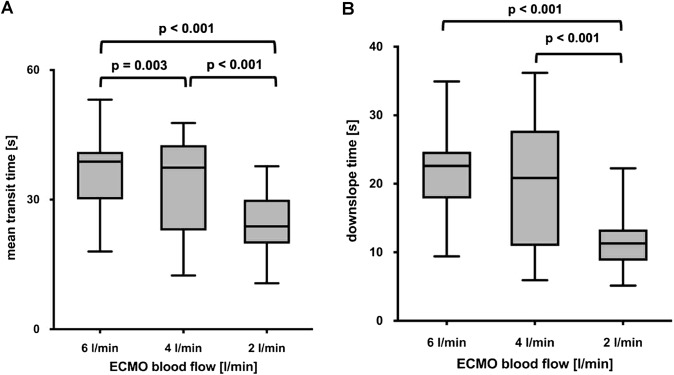
In severe acute respiratory distress syndrome (ARDS), veno-venous extracorporeal membrane oxygenation (V-V ECMO) has been proposed as a therapeutic strategy to possibly reduce mortality. Transpulmonary thermodilution (TPTD) enables monitoring of the extravascular lung water index (EVLWI) and cardiac preload parameters such as intrathoracic blood volume index (ITBVI) in patients with ARDS, but it is not generally recommended during V-V ECMO. We hypothesized that the amount of extracorporeal blood flow (ECBF) influences the calculation of EVLWI and ITBVI due to recirculation of indicator, which affects the measurement of the mean transit time (MTt), the time between injection and passing of half the indicator, as well as downslope time (DSt), the exponential washout of the indicator. EVLWI and ITBVI were measured in 20 patients with severe ARDS managed with V-V ECMO at ECBF rates from 6 to 4 and 2 l/min with TPTD. MTt and DSt significantly decreased when ECBF was reduced, resulting in a decreased EVLWI (26.1 [22.8-33.8] ml/kg at 6 l/min ECBF vs 22.4 [15.3-31.6] ml/kg at 4 l/min ECBF, p < 0.001; and 13.2 [11.8-18.8] ml/kg at 2 l/min ECBF, p < 0.001) and increased ITBVI (840 [753-1062] ml/m at 6 l/min ECBF vs 886 [658-979] ml/m at 4 l/min ECBF, p < 0.001; and 955 [817-1140] ml/m at 2 l/min ECBF, p < 0.001). In patients with severe ARDS managed with V-V ECMO, increasing ECBF alters the thermodilution curve, resulting in unreliable measurements of EVLWI and ITBVI. German Clinical Trials Register (DRKS00021050). Registered 14/08/2018. https://www.drks.de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00021050.
在严重急性呼吸窘迫综合征(ARDS)中,静脉-静脉体外膜肺氧合(V-V ECMO)已被提议作为一种治疗策略,以可能降低死亡率。经肺热稀释(TPTD)可监测 ARDS 患者的血管外肺水指数(EVLWI)和心脏前负荷参数,如胸腔内血容量指数(ITBVI),但一般不建议在 V-V ECMO 期间使用。我们假设由于指示剂的再循环,体外血液流量(ECBF)的量会影响 EVLWI 和 ITBVI 的计算,从而影响平均通过时间(MTt)的测量,即指示剂注射和通过一半的时间,以及下降时间(DSt),指示剂的指数洗脱。对 20 例接受 V-V ECMO 治疗的严重 ARDS 患者,在 ECBF 率为 6 至 4 和 2 l/min 时,用 TPTD 测量 EVLWI 和 ITBVI。当 ECBF 降低时,MTt 和 DSt 显著降低,导致 EVLWI 降低(6 l/min ECBF 时为 26.1 [22.8-33.8] ml/kg,4 l/min ECBF 时为 22.4 [15.3-31.6] ml/kg,p < 0.001;和 2 l/min ECBF 时为 13.2 [11.8-18.8] ml/kg,p < 0.001)和 ITBVI 增加(6 l/min ECBF 时为 840 [753-1062] ml/m,4 l/min ECBF 时为 886 [658-979] ml/m,p < 0.001;和 2 l/min ECBF 时为 955 [817-1140] ml/m,p < 0.001)。在接受 V-V ECMO 治疗的严重 ARDS 患者中,增加 ECBF 会改变热稀释曲线,导致 EVLWI 和 ITBVI 的测量不可靠。德国临床试验注册处(DRKS00021050)。注册于 2018 年 8 月 14 日。https://www.drks.de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00021050。