Department of Clinical Pharmacy and Pharmacology, University Medical Center Groningen, University of Groningen, the Netherlands.
Department of Anesthesiology, University Medical Center Groningen, University of Groningen, the Netherlands.
JAMA Netw Open. 2022 Oct 3;5(10):e2237970. doi: 10.1001/jamanetworkopen.2022.37970.
A variety of perioperative risk factors are associated with postoperative mortality risk. However, the relative contribution of routinely collected intraoperative clinical parameters to short-term and long-term mortality remains understudied.
To examine the performance of multiple machine learning models with data from different perioperative periods to predict 30-day, 1-year, and 5-year mortality and investigate factors that contribute to these predictions.
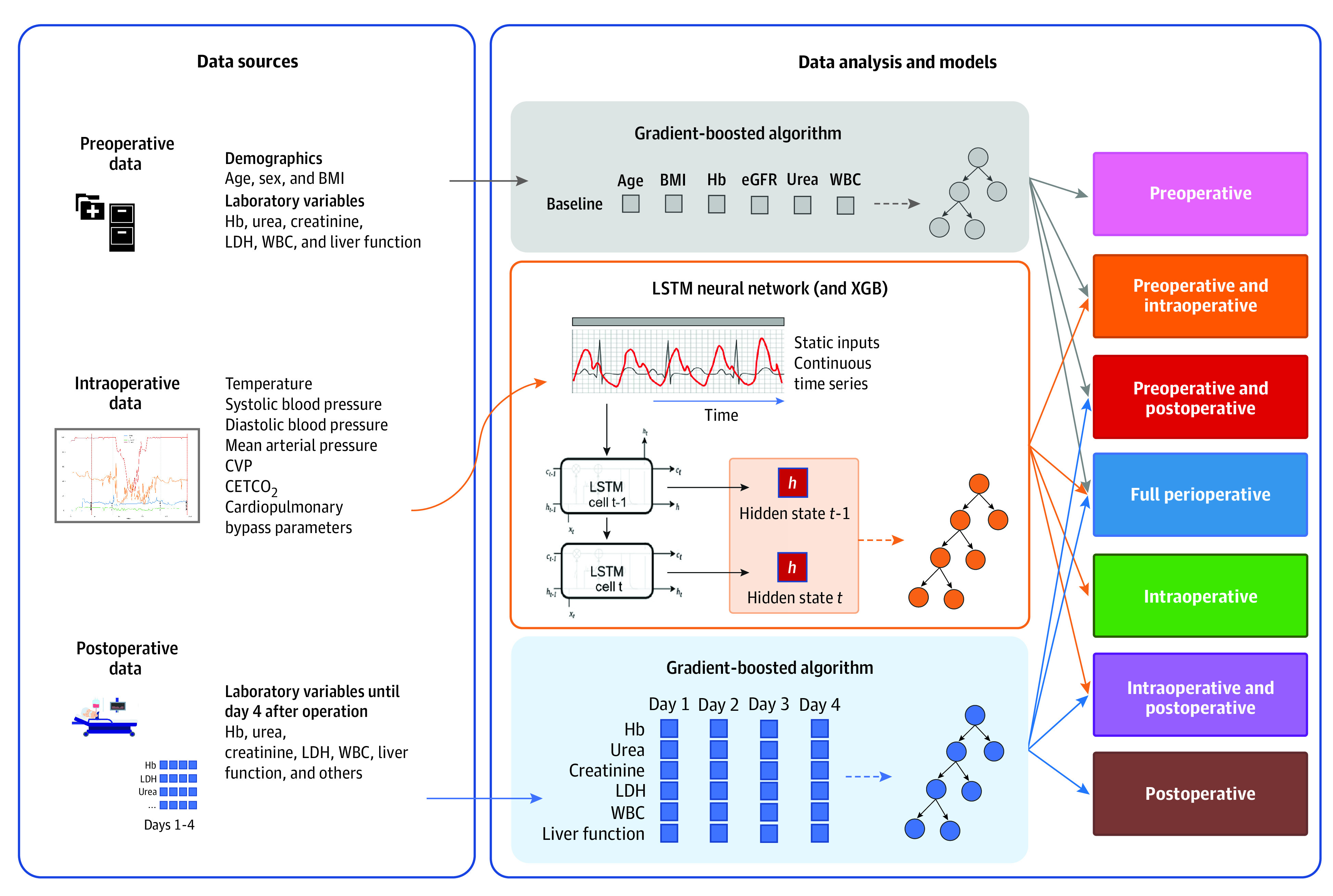
DESIGN, SETTING, AND PARTICIPANTS: In this prognostic study using prospectively collected data, risk prediction models were developed for short-term and long-term mortality after cardiac surgery. Included participants were adult patients undergoing a first-time valve operation, coronary artery bypass grafting, or a combination of both between 1997 and 2017 in a single center, the University Medical Centre Groningen in the Netherlands. Mortality data were obtained in November 2017. Data analysis took place between February 2020 and August 2021.
Cardiac surgery.
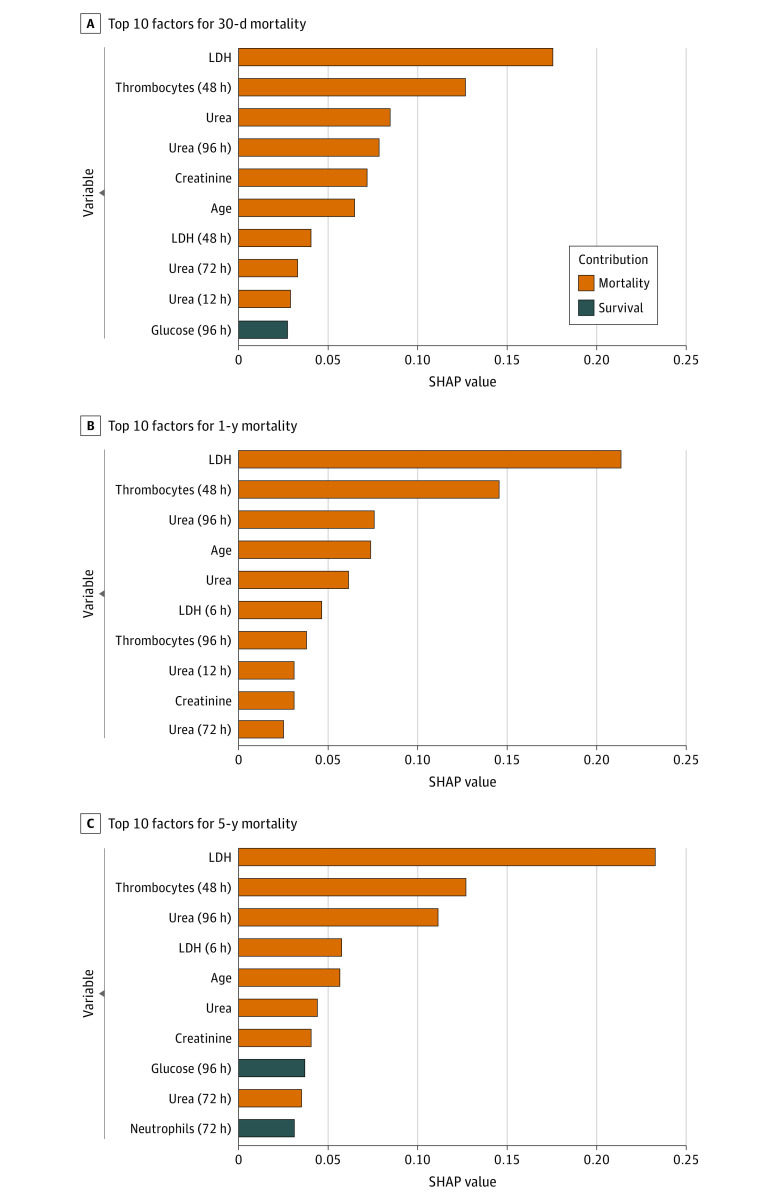
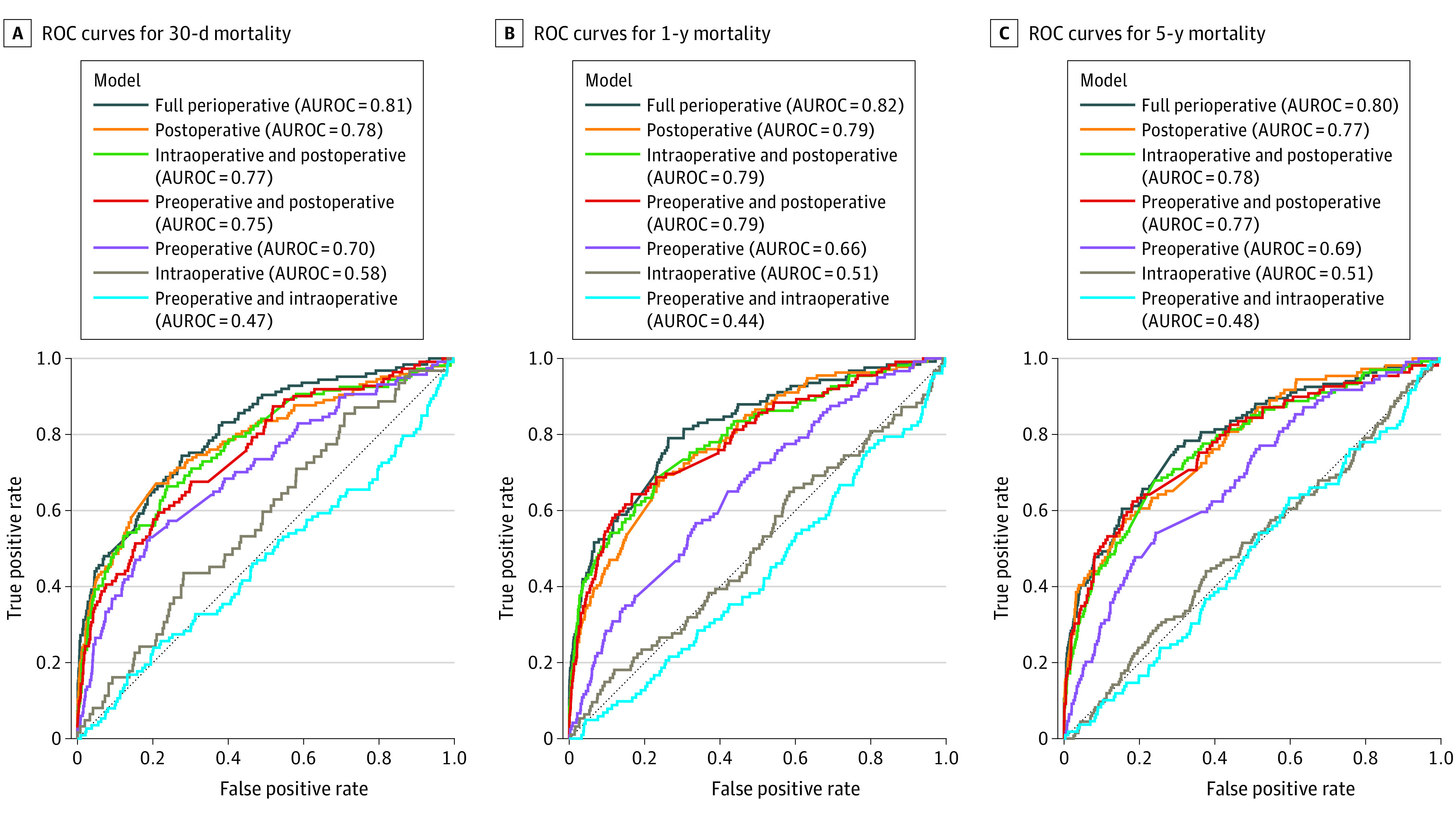
Postoperative mortality rates at 30 days, 1 year, and 5 years were the primary outcomes. The area under the receiver operating characteristic curve (AUROC) was used to assess discrimination. The contribution of all preoperative, intraoperative hemodynamic and temperature, and postoperative factors to mortality was investigated using Shapley additive explanations (SHAP) values.
Data from 9415 patients who underwent cardiac surgery (median [IQR] age, 68 [60-74] years; 2554 [27.1%] women) were included. Overall mortality rates at 30 days, 1 year, and 5 years were 268 patients (2.8%), 420 patients (4.5%), and 612 patients (6.5%), respectively. Models including preoperative, intraoperative, and postoperative data achieved AUROC values of 0.82 (95% CI, 0.78-0.86), 0.81 (95% CI, 0.77-0.85), and 0.80 (95% CI, 0.75-0.84) for 30-day, 1-year, and 5-year mortality, respectively. Models including only postoperative data performed similarly (30 days: 0.78 [95% CI, 0.73-0.82]; 1 year: 0.79 [95% CI, 0.74-0.83]; 5 years: 0.77 [95% CI, 0.73-0.82]). However, models based on all perioperative data provided less clinically usable predictions, with lower detection rates; for example, postoperative models identified a high-risk group with a 2.8-fold increase in risk for 5-year mortality (4.1 [95% CI, 3.3-5.1]) vs an increase of 11.3 (95% CI, 6.8-18.7) for the high-risk group identified by the full perioperative model. Postoperative markers associated with metabolic dysfunction and decreased kidney function were the main factors contributing to mortality risk.
This study found that the addition of continuous intraoperative hemodynamic and temperature data to postoperative data was not associated with improved machine learning-based identification of patients at increased risk of short-term and long-term mortality after cardiac operations.
各种围手术期风险因素与术后死亡率风险相关。然而,常规收集的术中临床参数对短期和长期死亡率的相对贡献仍研究不足。
研究使用不同围手术期数据的多种机器学习模型在预测心脏手术后 30 天、1 年和 5 年死亡率方面的表现,并探讨导致这些预测的因素。
设计、设置和参与者:这是一项使用前瞻性收集数据的预后研究,旨在为心脏手术后的短期和长期死亡率开发风险预测模型。纳入的参与者为 1997 年至 2017 年间在荷兰格罗宁根大学医学中心接受首次瓣膜手术、冠状动脉旁路移植术或两者结合的成年患者。在 2017 年 11 月获得死亡率数据。数据分析于 2020 年 2 月至 2021 年 8 月进行。
心脏手术。
30 天、1 年和 5 年的术后死亡率为主要结局。使用接收者操作特征曲线(AUROC)下面积评估区分度。使用 Shapley 加性解释(SHAP)值研究所有术前、术中血流动力学和体温以及术后因素对死亡率的贡献。
纳入了 9415 名接受心脏手术的患者(中位[IQR]年龄为 68 [60-74]岁;2554 [27.1%] 为女性)的数据。30 天、1 年和 5 年的总体死亡率分别为 268 例(2.8%)、420 例(4.5%)和 612 例(6.5%)。包括术前、术中、术后数据的模型在 30 天、1 年和 5 年的死亡率方面的 AUROC 值分别为 0.82(95%CI,0.78-0.86)、0.81(95%CI,0.77-0.85)和 0.80(95%CI,0.75-0.84)。仅包含术后数据的模型表现类似(30 天:0.78 [95%CI,0.73-0.82];1 年:0.79 [95%CI,0.74-0.83];5 年:0.77 [95%CI,0.73-0.82])。然而,基于所有围手术期数据的模型提供了预测性较差的结果,检测率较低;例如,术后模型确定了一个 5 年死亡率风险增加 2.8 倍的高危组(4.1 [95%CI,3.3-5.1]),而全围手术期模型确定的高危组风险增加了 11.3(95%CI,6.8-18.7)。与代谢功能障碍和肾脏功能下降相关的术后标志物是导致死亡率风险的主要因素。
本研究发现,将术中连续血流动力学和体温数据添加到术后数据中并不能提高基于机器学习的识别心脏手术后短期和长期死亡率风险增加患者的能力。