Piccirillo Gianfranco, Moscucci Federica, Corrao Andrea, Carnovale Myriam, Di Diego Ilaria, Lospinuso Ilaria, Caltabiano Cristina, Mezzadri Martina, Rossi Pietro, Magrì Damiano
Department of Internal and Clinical Medicine, Anesthesiology and Cardiovascular Sciences, Policlinico Umberto I, "Sapienza" University of Rome, Viale del Policlinico n. 155, 00186 Rome, Italy.
Arrhytmology Unit, Cardiology Division, S. Giovanni Calibita, Isola Tiberina, 00186 Rome, Italy.
Biomedicines. 2022 Sep 26;10(10):2407. doi: 10.3390/biomedicines10102407.
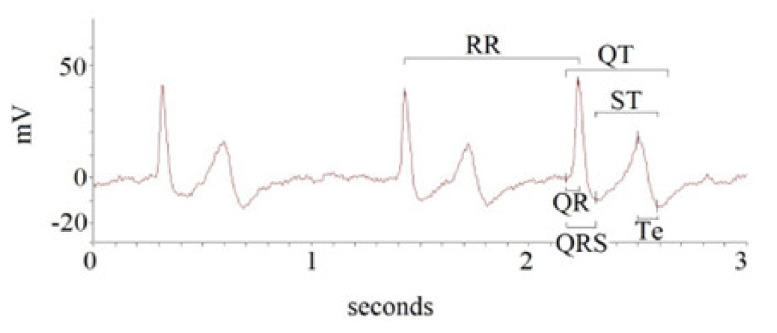
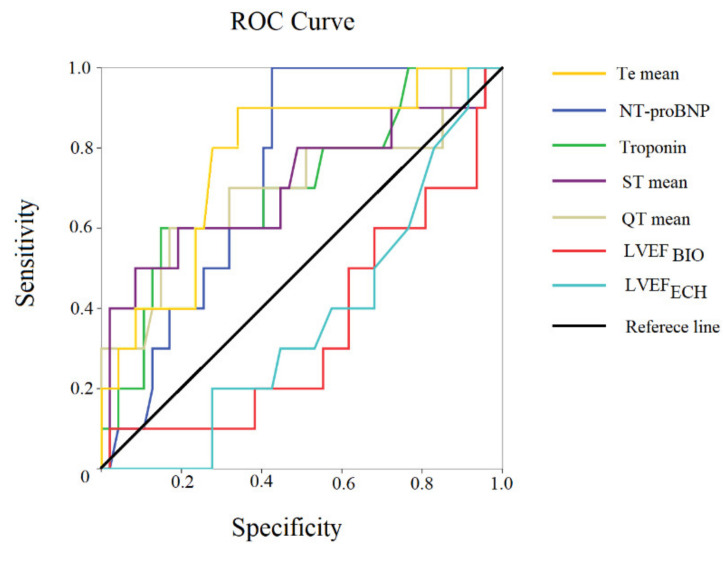
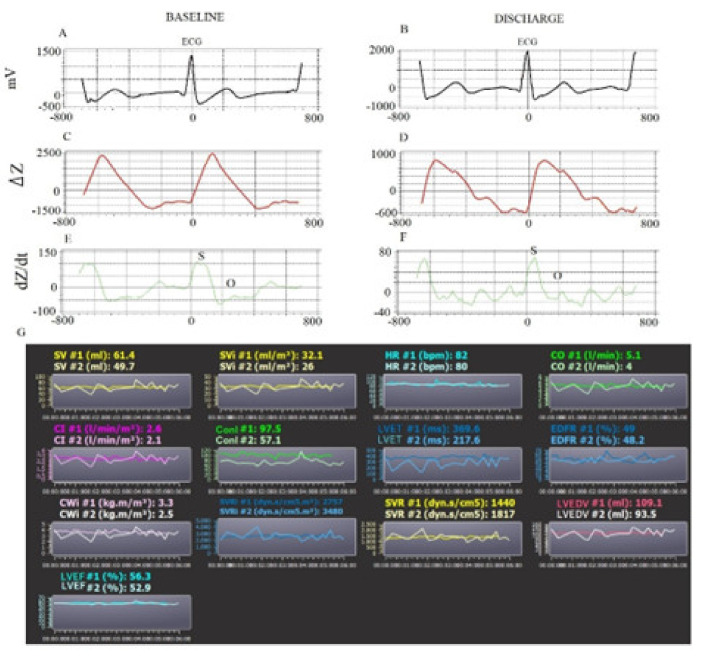
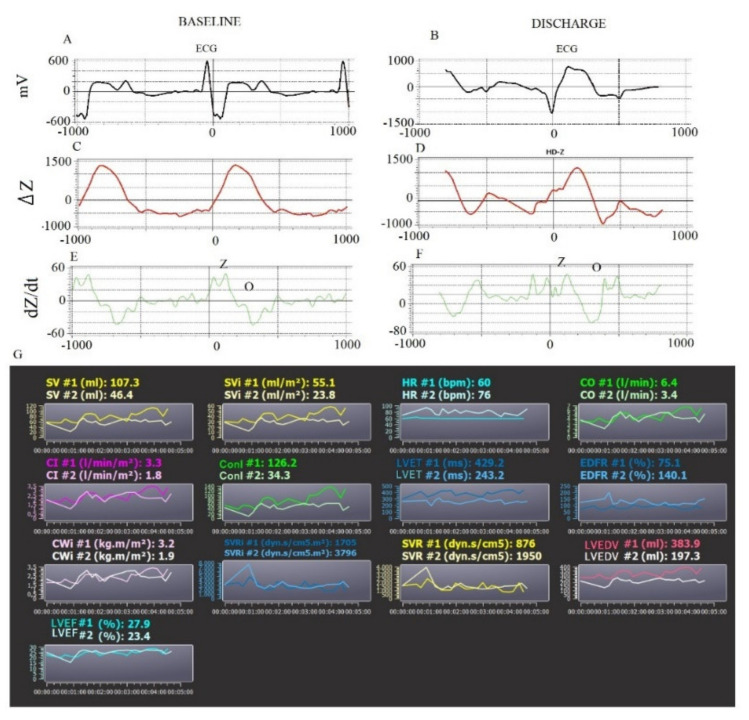
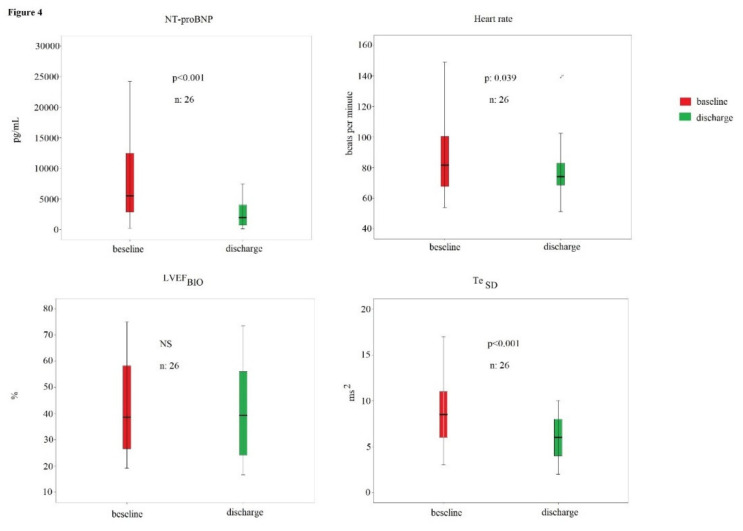
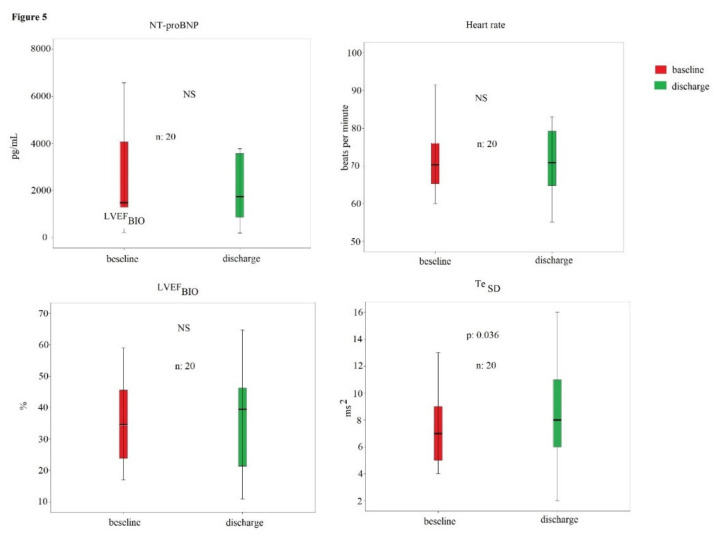
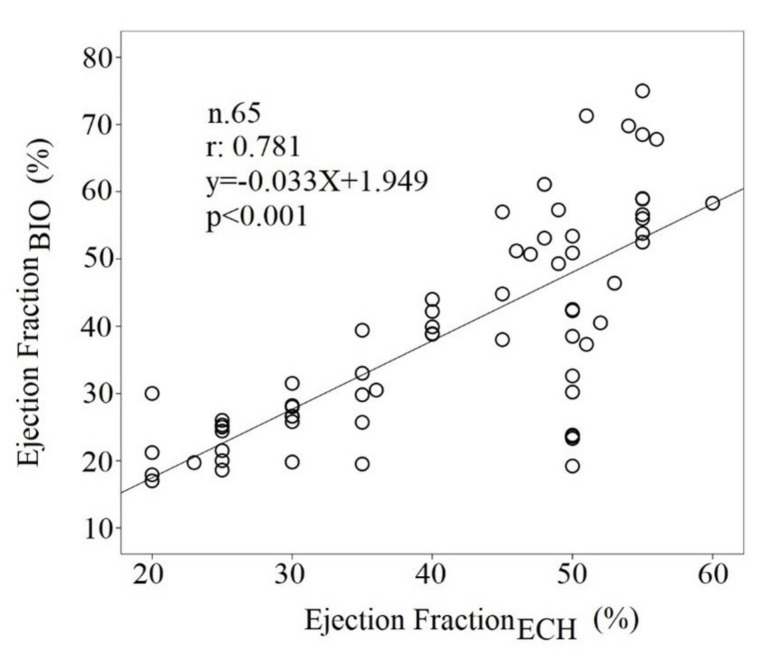
Using bio-impedance to deduce some hemodynamic parameters combined with some short-term ECG temporal dispersion intervals, and measuring myocardial depolarization, intraventricular conduction, and repolarization. A total of 65 in-hospital patients (M/F:35/30) were enrolled, 39 with HFrEF and 26 HFpEF, in New York Heart Association (NYHA) class IV. Stroke volume (SVI), cardiac indexes (CI), left ventricular ejection fraction (LVEFBIO), end diastolic volume (LV-EDV), and other systolic and diastolic parameters were noninvasively obtained at enrollment and at hospital discharge. At the same time, QR, QRS, QT, ST, Tpeak-Tend (Te) interval mean, and standard deviation (SD) from 5 min ECG recordings were obtained. At baseline, HFrEF patients reported significantly lower SVI (p < 0.05), CI (p < 0.05), and LVEF (p < 0.001) than HFpEF patients; moreover, HFrEF patients also showed increased LV-EDV (p < 0.05), QR, QRS, QT, ST, and Te means (p < 0.05) and standard deviations (p < 0.05) in comparison to HFpEF subjects. Multivariable logistic regression analysis reported a significant correlation between hospital mortality and Te mean (odds ratio: 1.03, 95% confidence limit: 1.01−1.06, p: 0.01). Fifty-seven percent of patients were considered responders to optimal medical therapy and, at discharge, they had significantly reduced NT-proBNP, (p < 0.001), heart rate (p < 0.05), and TeSD (p < 0.001). LVEF, obtained by transthoracic echocardiography, and LVEFBIO were significantly related (r: 0.781, p < 0.001), but these two parameters showed a low agreement limit. Noninvasive hemodynamic and ECG-derived parameters were useful to highlight the difference between HFrEF and HFpEF and between responders and nonresponders to the optimal medical therapy. Short-period bioimpedance and electrocardiographic data should be deeply evaluated to determine possible advantages in the therapeutic and prognostic approach in severe CHF.
利用生物阻抗结合一些短期心电图时间离散间期来推导一些血流动力学参数,并测量心肌去极化、心室内传导和复极化。共纳入65例住院患者(男/女:35/30),纽约心脏协会(NYHA)心功能IV级,其中39例为射血分数降低的心力衰竭(HFrEF)患者,26例为射血分数保留的心力衰竭(HFpEF)患者。在入院时和出院时无创获取每搏输出量(SVI)、心脏指数(CI)、左心室射血分数(LVEFBIO)、舒张末期容积(LV-EDV)以及其他收缩和舒张参数。同时,从5分钟心电图记录中获取QR、QRS、QT、ST、Tpeak-Tend(Te)间期均值和标准差(SD)。基线时,HFrEF患者的SVI(p < 0.05)、CI(p < 0.05)和LVEF(p < 0.001)显著低于HFpEF患者;此外,与HFpEF患者相比,HFrEF患者的LV-EDV(p < 0.05)、QR、QRS、QT、ST和Te均值(p < 0.05)及标准差(p < 0.05)也有所增加。多变量逻辑回归分析显示,医院死亡率与Te均值之间存在显著相关性(比值比:1.03,95%置信区间:1.01−1.06,p:0.01)。57%的患者被认为对最佳药物治疗有反应,出院时,他们的N末端B型利钠肽原(NT-proBNP)(p < 0.001)、心率(p < 0.05)和TeSD(p < 0.001)显著降低。经胸超声心动图测得的LVEF与LVEFBIO显著相关(r:0.781,p < 0.001),但这两个参数的一致性界限较低。无创血流动力学和心电图衍生参数有助于突出HFrEF和HFpEF之间以及最佳药物治疗反应者和无反应者之间的差异。应深入评估短期生物阻抗和心电图数据,以确定其在重度慢性心力衰竭治疗和预后方法中的潜在优势。