O'Neal Wesley T, Mazur Matylda, Bertoni Alain G, Bluemke David A, Al-Mallah Mouaz H, Lima Joao A C, Kitzman Dalane, Soliman Elsayed Z
Division of Cardiology, Department of Medicine, Emory University School of Medicine, Atlanta, GA.
Department of Internal Medicine, Wake Forest School of Medicine, Winston-Salem, NC.
J Am Heart Assoc. 2017 May 25;6(6):e006023. doi: 10.1161/JAHA.117.006023.
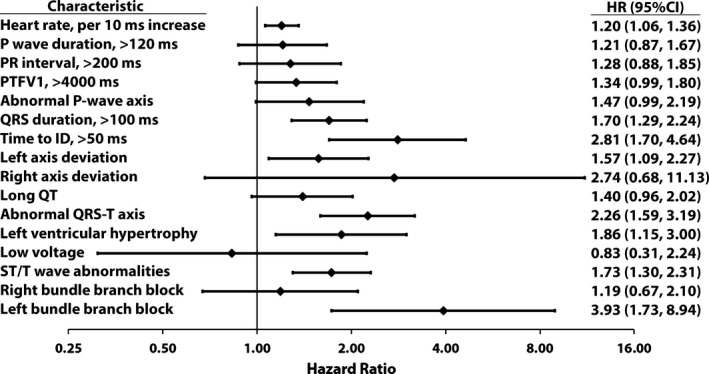
Several markers detected on the routine 12-lead ECG are associated with future heart failure events. We examined whether these markers are able to separate the risk of heart failure with reduced ejection fraction (HFrEF) from heart failure with preserved ejection fraction (HFpEF).
We analyzed data of 6664 participants (53% female; mean age 62±10 years) from MESA (Multi-Ethnic Study of Atherosclerosis) who were free of cardiovascular disease at baseline (2000-2002). A competing risks analysis was used to compare the association of several baseline ECG predictors with HFrEF and HFpEF detected during a median follow-up of 12.1 years. A total of 127 HFrEF and 117 HFpEF events were detected during follow-up. In a multivariable adjusted model, prolonged QRS duration, delayed intrinsicoid deflection, left-axis deviation, right-axis deviation, prolonged QT interval, abnormal QRS-T axis, left ventricular hypertrophy, ST/T-wave abnormalities, and left bundle-branch block were associated with HFrEF. In contrast, higher resting heart rate, abnormal P-wave axis, and abnormal QRS-T axis were associated with HFpEF. The risk of HFrEF versus HFpEF was significantly differently for delayed intrinsicoid deflection (hazard ratio: 4.90 [95% confidence interval (CI), 2.77-8.68] versus 0.94 [95% CI, 0.29-2.97]; comparison =0.013), prolonged QT interval (hazard ratio: 2.39 [95% CI, 1.55-3.68] versus 0.52 [95% CI, 0.23-1.19]; comparison <0.001), and ST/T-wave abnormalities (hazard ratio: 2.47 [95% CI, 1.69-3.62] versus 1.13 [95% CI, 0.72-1.77]; comparison =0.0093).
Markers of ventricular repolarization and delayed ventricular activation are able to distinguish between the future risk of HFrEF and HFpEF. These findings suggest a role for ECG markers in the personalized risk assessment of heart failure subtypes.
在常规12导联心电图上检测到的几种标志物与未来心力衰竭事件相关。我们研究了这些标志物是否能够区分射血分数降低的心力衰竭(HFrEF)和射血分数保留的心力衰竭(HFpEF)的风险。
我们分析了来自动脉粥样硬化多族裔研究(MESA)的6664名参与者(53%为女性;平均年龄62±10岁)的数据,这些参与者在基线时(2000 - 2002年)无心血管疾病。采用竞争风险分析比较几种基线心电图预测指标与在中位随访12.1年期间检测到的HFrEF和HFpEF的关联。随访期间共检测到127例HFrEF事件和117例HFpEF事件。在多变量调整模型中,QRS时限延长、类本位曲折延迟、电轴左偏、电轴右偏、QT间期延长、QRS - T电轴异常、左心室肥厚、ST/T波异常和左束支传导阻滞与HFrEF相关。相比之下,静息心率升高、P波电轴异常和QRS - T电轴异常与HFpEF相关。类本位曲折延迟时HFrEF与HFpEF的风险存在显著差异(风险比:4.90 [95%置信区间(CI),2.77 - 8.68] 对比 0.94 [95% CI,0.29 - 2.97];比较P = 0.013),QT间期延长时(风险比:2.39 [95% CI,1.55 - 3.68] 对比 0.52 [95% CI,0.23 - 1.19];比较P < 0.001),以及ST/T波异常时(风险比:2.47 [95% CI,1.69 - 3.62] 对比 1.13 [95% CI,0.72 - 1.77];比较P = 0.0093)。
心室复极和心室激活延迟的标志物能够区分HFrEF和HFpEF的未来风险。这些发现提示心电图标志物在心力衰竭亚型的个性化风险评估中具有作用。