Omar Mahmoud, Attia Abdallah S, Issa Peter P, Christensen Bryce R, Sugumar Kavin, Alnahla Ahmed, Hadedeya Deena, Shalaby Hosam, Gupta Neel, Shama Mohamed, Toraih Eman, Kandil Emad
Department of Surgery, School of Medicine, Tulane University, New Orleans, LA 70112, USA.
School of Medicine, Louisiana State University Health Sciences Center, New Orleans, LA 70112, USA.
Biomedicines. 2022 Sep 26;10(10):2408. doi: 10.3390/biomedicines10102408.
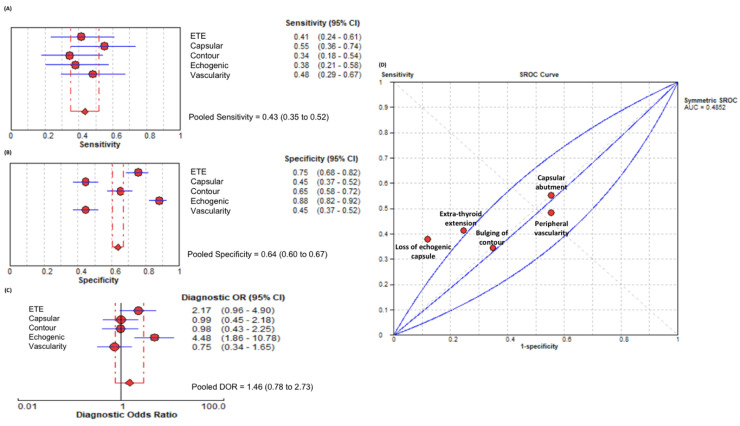
Detection of extrathyroidal extension (ETE) in patients with papillary thyroid carcinoma (PTC) influences treatment plan and surgical aggressiveness. Ultrasound (US) is the long-standing preoperative imaging method of choice. Recent literature from Asia suggests US accuracy to be influenced by patient characteristics, such as body mass index (BMI). Here, we examine the effect of BMI on the accuracy of US at a North American tertiary referral center. A total of 204 PTC-confirmed patients were retrospectively read by a radiologist blinded to surgical pathology findings. The radiologist recorded multiple sonographic features, including ETE, loss of echogenic capsule, nodule vascularity, capsular abutment, and bulging of contour. When considering all patients, the ultrasonographic feature with the best overall performance was loss of echogenic capsule (diagnostic odds ratio (DOR) = 4.48, 95% confidence interval (CI) = 1.86-10.78). Sub-group analysis by patient BMI found that area under the curve (AUC) for sonographic features was greater in non-obese BMI patients (0.71 ± 0.06) when compared with obese patients (0.43 ± 0.05; = 0.001). Overall, US diagnostic performance was significantly better in non-obese (DOR = 3.70, 95%CI = 1.53-8.94) patients when compared to those who were obese (DOR = 1.12, 95%CI = 0.62-2.03; = 0.03). Loss of the echogenic capsule did not differ between the two cohorts with respect to DOR ( = 0.51), specificity ( = 0.52), or sensitivity ( = 0.09). Our work suggests that the diagnostic value of ETE detection by US is impaired in obese patients. Considering that loss of the echogenic capsule did not differ with respect to diagnostic performance, specificity, nor sensitivity between non-obese and obese patients, it could be considered the most important predictor of US-determined ETE.
检测甲状腺乳头状癌(PTC)患者的甲状腺外侵犯(ETE)会影响治疗方案和手术的激进程度。超声(US)是长期以来首选的术前成像方法。亚洲最近的文献表明,超声的准确性受患者特征的影响,如体重指数(BMI)。在此,我们在北美一家三级转诊中心研究BMI对超声准确性的影响。一位对手术病理结果不知情的放射科医生对总共204例确诊为PTC的患者进行了回顾性阅片。放射科医生记录了多个超声特征,包括ETE、低回声包膜消失、结节血管形成、包膜毗邻和轮廓隆起。在考虑所有患者时,总体表现最佳的超声特征是低回声包膜消失(诊断比值比(DOR)=4.48,95%置信区间(CI)=1.86 - 10.78)。按患者BMI进行亚组分析发现,与肥胖患者(0.43±0.05;P = 0.001)相比,非肥胖BMI患者超声特征的曲线下面积(AUC)更大(0.71±0.06)。总体而言,与肥胖患者(DOR = 1.12,95%CI = 0.62 - 2.03;P = 0.03)相比,非肥胖患者(DOR = 3.70,95%CI = 1.53 - 8.94)的超声诊断性能明显更好。两个队列在低回声包膜消失方面的DOR(P = 0.51)、特异性(P = 0.52)或敏感性(P = 0.09)没有差异。我们的研究表明,肥胖患者中超声检测ETE的诊断价值受损。鉴于非肥胖和肥胖患者在低回声包膜消失方面的诊断性能、特异性和敏感性没有差异,它可被视为超声确定的ETE的最重要预测指标。