Bobot Mickaël, Tonon David, Peres Noémie, Guervilly Christophe, Lefèvre Flora, Max Howard, Bommel Youri, Volff Maxime, Leone Marc, Lopez Alexandre, Simeone Pierre, Carvelli Julien, Chopinet Sophie, Hraiech Sami, Papazian Laurent, Velly Lionel, Bourenne Jérémy, Forel Jean-Marie
Centre de Néphrologie et Transplantation Rénale, Hôpital de la Conception, AP-HM, 13005 Marseille, France.
Aix Marseille University, INSERM 1263, INRAE 1260, C2VN, European Center for Medical Imaging Research (CERIMED), Campus Santé Timone, 13005 Marseille, France.
J Clin Med. 2022 Oct 18;11(20):6130. doi: 10.3390/jcm11206130.
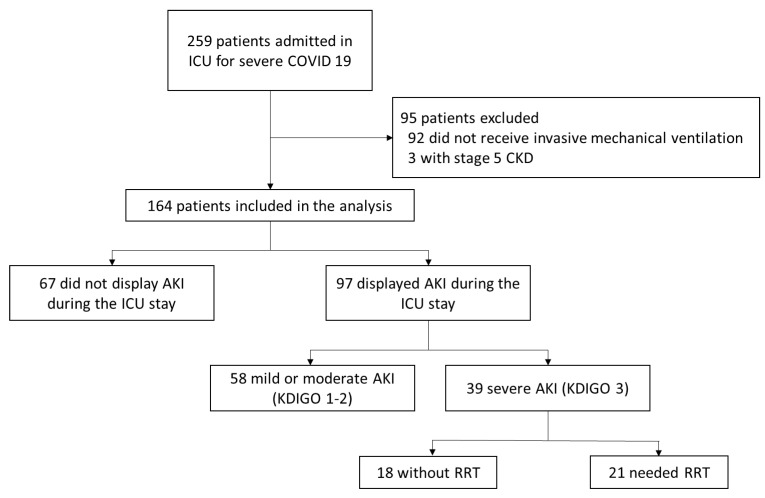
Background: Acute kidney injury (AKI) is the second most frequent condition after acute respiratory distress syndrome (ARDS) in critically ill patients with severe COVID-19 and is strongly associated with mortality. The aim of this multicentric study was to assess the impact of the specific treatments of COVID-19 and ARDS on the risk of severe AKI in critically ill COVID-19 patients. Methods: In this cohort study, data from consecutive patients older than 18 years admitted to 6 ICUs for COVID-19-related ARDS requiring invasive mechanical ventilation were included. The incidence and severity of AKI, defined according to the 2012 KDIGO definition, were monitored during the entire ICU stay until day 90. Patients older than 18 years admitted to the ICU for COVID-19-related ARDS requiring invasive mechanical ventilation were included. Results: 164 patients were included in the final analysis; 97 (59.1%) displayed AKI, of which 39 (23.8%) had severe stage 3 AKI, and 21 (12.8%) required renal replacement therapy (RRT). In univariate analysis, severe AKI was associated with angiotensin-converting enzyme inhibitors (ACEI) exposure (p = 0.016), arterial hypertension (p = 0.029), APACHE-II score (p = 0.004) and mortality at D28 (p = 0.008), D60 (p < 0.001) and D90 (p < 0.001). In multivariate analysis, the factors associated with the onset of stage 3 AKI were: exposure to ACEI (OR: 4.238 (1.307−13.736), p = 0.016), APACHE II score (without age) (OR: 1.138 (1.044−1.241), p = 0.003) and iNO (OR: 5.694 (1.953−16.606), p = 0.001). Prone positioning (OR: 0.234 (0.057−0.967), p = 0.045) and dexamethasone (OR: 0.194 (0.053−0.713), p = 0.014) were associated with a decreased risk of severe AKI. Conclusions: Dexamethasone was associated with the prevention of the risk of severe AKI and RRT, and iNO was associated with severe AKI and RRT in critically ill patients with COVID-19. iNO should be used with caution in COVID-19-related ARDS.
在患有严重新型冠状病毒肺炎(COVID-19)的危重症患者中,急性肾损伤(AKI)是仅次于急性呼吸窘迫综合征(ARDS)的第二常见病症,且与死亡率密切相关。这项多中心研究的目的是评估COVID-19和ARDS的特定治疗方法对危重症COVID-19患者发生严重AKI风险的影响。方法:在这项队列研究中,纳入了因COVID-19相关ARDS入住6个重症监护病房(ICU)且需要有创机械通气的18岁以上连续患者的数据。根据2012年改善全球肾脏病预后组织(KDIGO)的定义对AKI的发病率和严重程度进行监测,直至ICU住院第90天。纳入因COVID-19相关ARDS入住ICU且需要有创机械通气的18岁以上患者。结果:164例患者纳入最终分析;97例(59.1%)出现AKI,其中39例(23.8%)为严重3期AKI,21例(12.8%)需要肾脏替代治疗(RRT)。在单因素分析中,严重AKI与血管紧张素转换酶抑制剂(ACEI)暴露(p = 0.016)、动脉高血压(p = 0.029)、急性生理与慢性健康状况评分系统II(APACHE-II)评分(p = 0.004)以及第28天(p = 0.008)、第60天(p < 0.001)和第90天(p < 0.001)的死亡率相关。在多因素分析中,与3期AKI发生相关的因素为:ACEI暴露(比值比:4.238(1.307 - 13.736),p = 0.016)、APACHE II评分(不包括年龄)(比值比:1.138(1.044 - 1.241),p = 0.003)和吸入一氧化氮(iNO)(比值比:5.694(1.953 - 16.606),p = 0.001)。俯卧位(比值比:0.234(0.057 - 0.967),p = 0.045)和地塞米松(比值比:0.194(0.053 - 0.713),p = 0.014)与严重AKI风险降低相关。结论:地塞米松与预防危重症COVID-19患者发生严重AKI和RRT的风险相关,而iNO与危重症COVID-19患者的严重AKI和RRT相关。在COVID-19相关ARDS中应谨慎使用iNO。