Baroutidou Amalia, Kartas Anastasios, Papazoglou Andreas S, Kosmidis Diamantis, Moysidis Dimitrios V, Otountzidis Nikolaos, Doundoulakis Ioannis, Despotopoulos Stefanos, Vrana Elena, Koutsakis Athanasios, Rampidis Georgios P, Ntiloudi Despoina, Liori Sotiria, Avramidis Dimosthenis, Karagiannidis Efstratios, Nikolopoulos Theodoros Thomas, Apostolopoulou Sotiria, Frogoudaki Alexandra, Tzifa Afrodite, Karvounis Haralambos, Giannakoulas George
First Department of Cardiology, AHEPA University Hospital, Aristotle University of Thessaloniki, St. Kiriakidi 1, 54636 Thessaloniki, Greece.
Department of Pediatric and Adult Congenital Heart Disease, Onassis Cardiac Surgery Center, 17674 Athens, Greece.
J Clin Med. 2022 Oct 20;11(20):6181. doi: 10.3390/jcm11206181.
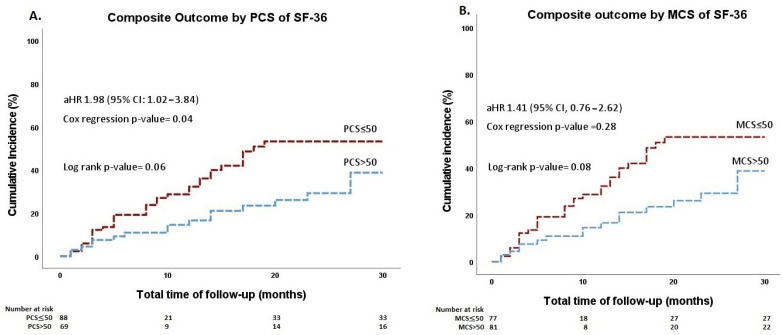
The prognostic value of health status metrics in patients with adult congenital heart disease (ACHD) and atrial arrhythmias is unclear. In this retrospective cohort study of an ongoing national, multicenter registry (PROTECT-AR, NCT03854149), ACHD patients with atrial arrhythmias on apixaban are included. At baseline, health metrics were assessed using the physical component summary (PCS), the mental component summary (MCS) of the Short-Form-36 (SF-36) Health Survey, and the modified European Heart Rhythm Association (mEHRA) score. Patients were divided into groups according to their SF-36 PCS and MCS scores, using the normalized population mean of 50 on the PCS and MCS as a threshold. The primary outcome was the composite of mortality from any cause, major thromboembolic events, major/clinically relevant non-major bleedings, or hospitalizations. Multivariable Cox-regression analyses using clinically relevant parameters (age greater than 60 years, anatomic complexity, ejection fraction of the systemic ventricle, and CHA₂DS₂-VASc and HAS-BLED scores) were performed to examine the association of health metrics with the composite outcome. Over a median follow-up period of 20 months, the composite outcome occurred in 50 of 158 (32%) patients. The risk of the outcome was significantly higher in patients with SF-36 PCS ≤ 50 compared with those with PCS > 50 (adjusted hazard ratio (aHR), 1.98; 95% confidence interval [CI], 1.02−3.84; p = 0.04) after adjusting for possible confounders. The SF-36 MCS ≤ 50 was not associated with the outcome. The mEHRA score was incrementally associated with a higher risk of the composite outcome (aHR = 1.44 per 1 unit increase in score; 95% CI, 1.03−2.00; p = 0.03) in multivariable analysis. In ACHD patients with atrial arrhythmias, the SF-36 PCS ≤ 50 and mEHRA scores predicted an increased risk of adverse events.
健康状况指标对成人先天性心脏病(ACHD)合并房性心律失常患者的预后价值尚不清楚。在这项对正在进行的全国性多中心注册研究(PROTECT-AR,NCT03854149)的回顾性队列研究中,纳入了接受阿哌沙班治疗的合并房性心律失常的ACHD患者。在基线时,使用简明健康调查量表(SF-36)的身体成分总结(PCS)、精神成分总结(MCS)以及改良的欧洲心律协会(mEHRA)评分来评估健康指标。根据患者的SF-36 PCS和MCS评分进行分组,将PCS和MCS的标准化总体均值50作为阈值。主要结局是任何原因导致的死亡、重大血栓栓塞事件、重大/临床相关非重大出血或住院的复合结局。使用临床相关参数(年龄大于60岁、解剖复杂性、体循环心室射血分数以及CHA₂DS₂-VASc和HAS-BLED评分)进行多变量Cox回归分析,以检验健康指标与复合结局之间的关联。在中位随访期20个月内,158例患者中有50例(32%)出现了复合结局。在调整可能的混杂因素后,SF-36 PCS≤50的患者发生结局的风险显著高于PCS>50的患者(调整后风险比[aHR],1.98;95%置信区间[CI],1.02−3.84;p = 0.04)。SF-36 MCS≤50与结局无关。在多变量分析中,mEHRA评分每增加1个单位,复合结局的风险就会相应增加(aHR = 1.44;95%CI,1.03−2.00;p = 0.03)。在合并房性心律失常的ACHD患者中,SF-36 PCS≤50和mEHRA评分预示不良事件风险增加。