Sanderson Peter A, Esnal-Zufiaurre Arantza, Arends Mark J, Herrington C Simon, Collins Frances, Williams Alistair R W, Saunders Philippa T K
Centre for Inflammation Research, Edinburgh Bioquarter, The University of Edinburgh, Edinburgh, United Kingdom.
Cancer Research UK Edinburgh Centre, Institute of Genetics and Cancer, Western General Hospital, The University of Edinburgh, Edinburgh, United Kingdom.
Front Reprod Health. 2022 May 12;4:896170. doi: 10.3389/frph.2022.896170. eCollection 2022.
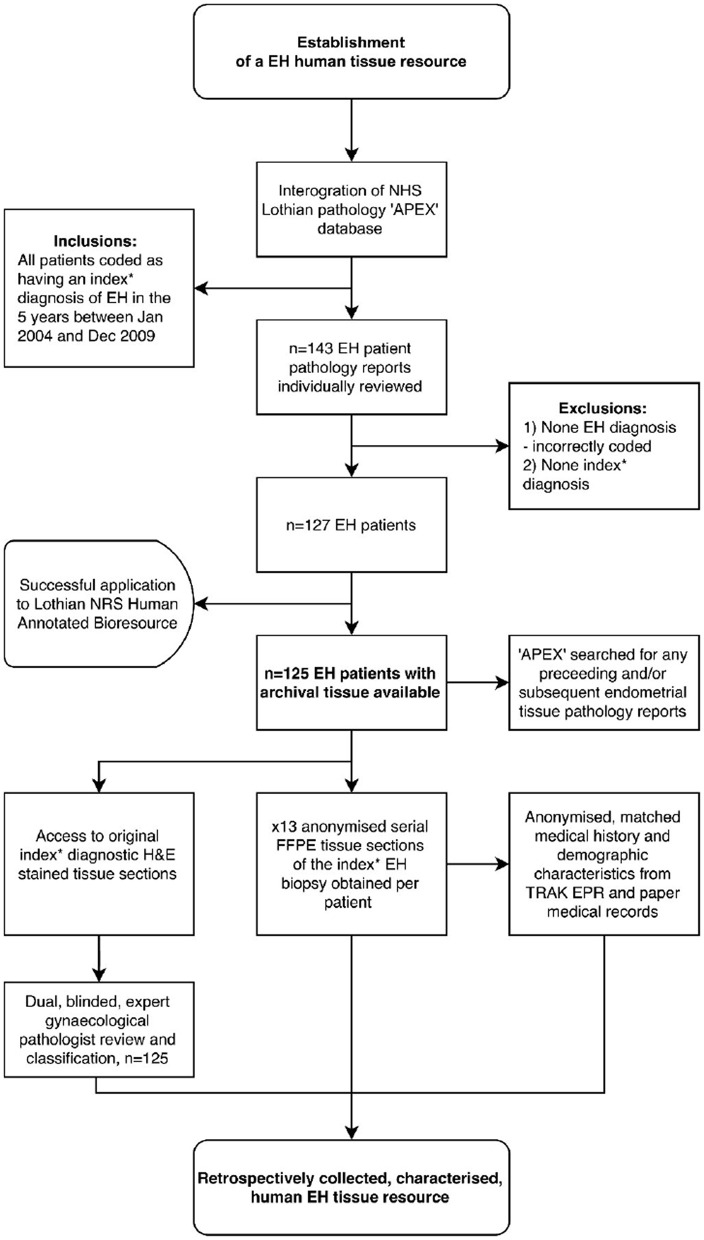
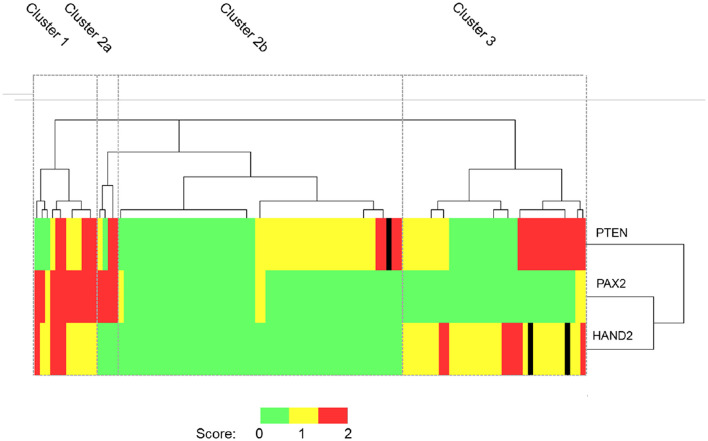
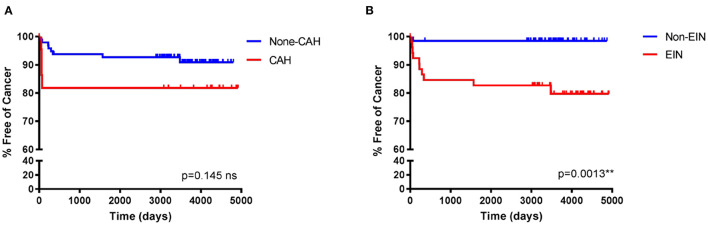
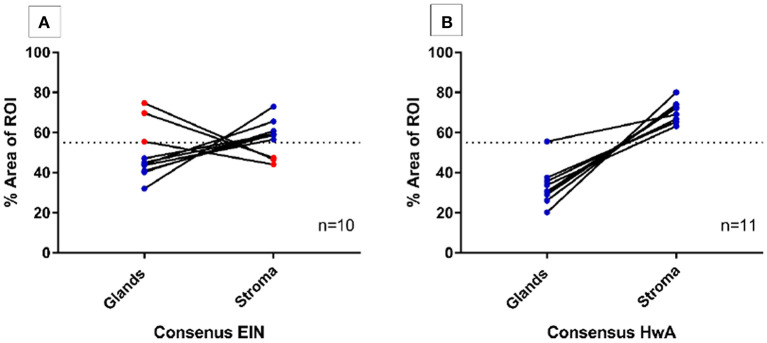
Endometrial hyperplasia (EH) is a precursor lesion to endometrial carcinoma (EC). Risks for EC include genetic, hormonal and metabolic factors most notably those associated with obesity: rates are rising and there is concern that cases in pre-menopausal women may remain undetected. Making an accurate distinction between benign and pre-malignant disease is both a challenge for the pathologist and important to the gynecologist who wants to deliver the most appropriate care to meet the needs of the patient. Premalignant change may be recognized by histological changes of endometrial hyperplasia (which may occur with or without atypia) and endometrial intraepithelial neoplasia (EIN). In this study we created a tissue resource of EH samples diagnosed between 2004 and 2009 ( = 125) and used this to address key questions: 1. Are the EIN/WHO2014 diagnostic criteria able to consistently identify premalignant endometrium? 2. Can computer aided image analysis inform identification of EIN? 3. Can we improve diagnosis by incorporating analysis of protein expression using immunohistochemistry. Our findings confirmed the inclusion of EIN in diagnostic criteria resulted in a better agreement between expert pathologists compared with the previous WHO94 criteria used for the original diagnosis of our sample set. A computer model based on assessment of stromal:epithelial ratio appeared most accurate in classification of areas of tissue without EIN. From an extensive panel of putative endometrial protein tissue biomarkers a score based on assessment of HAND2, PTEN, and PAX2 was able to identify four clusters one of which appeared to be more likely to be benign. In summary, our study has highlighted new opportunities to improve diagnosis of pre-malignant disease in endometrium and provide a platform for further research on this important topic.
子宫内膜增生(EH)是子宫内膜癌(EC)的前驱病变。EC的风险包括遗传、激素和代谢因素,其中最显著的是与肥胖相关的因素:其发病率正在上升,人们担心绝经前女性的病例可能仍未被发现。准确区分良性和癌前疾病对病理学家来说是一项挑战,对希望提供最恰当治疗以满足患者需求的妇科医生来说也很重要。癌前变化可通过子宫内膜增生的组织学变化(可伴有或不伴有异型性)以及子宫内膜上皮内瘤变(EIN)来识别。在本研究中,我们创建了一个2004年至2009年间诊断的EH样本组织资源库(n = 125),并以此来解决关键问题:1. EIN/WHO2014诊断标准能否始终如一地识别癌前子宫内膜?2. 计算机辅助图像分析能否有助于识别EIN?3. 我们能否通过纳入免疫组织化学对蛋白质表达的分析来改善诊断?我们的研究结果证实,与用于我们样本集原始诊断的先前WHO94标准相比,将EIN纳入诊断标准可使专家病理学家之间的一致性更好。基于间质与上皮比例评估的计算机模型在无EIN的组织区域分类中似乎最为准确。从大量假定的子宫内膜蛋白质组织生物标志物中,基于HAND2、PTEN和PAX2评估得出的一个分数能够识别出四个簇,其中一个簇似乎更可能是良性的。总之,我们的研究突出了改善子宫内膜癌前疾病诊断的新机会,并为这一重要课题的进一步研究提供了一个平台。