Lens Sabela, Miralpeix Anna, Gálvez Mont, Martró Elisa, González Noemi, Rodríguez-Tajes Sergio, Mariño Zoe, Saludes Verónica, Reyes-Urueña Juliana, Majó Xavier, Colom Joan, Forns Xavier
Liver Unit, Hospital Clínic, IDIBAPS, Universitat de Barcelona, Barcelona, Spain.
Biomedical Research Networking Centre in Liver and Digestive Diseases (CIBEREHD), Madrid, Spain.
JHEP Rep. 2022 Sep 13;4(12):100580. doi: 10.1016/j.jhepr.2022.100580. eCollection 2022 Dec.
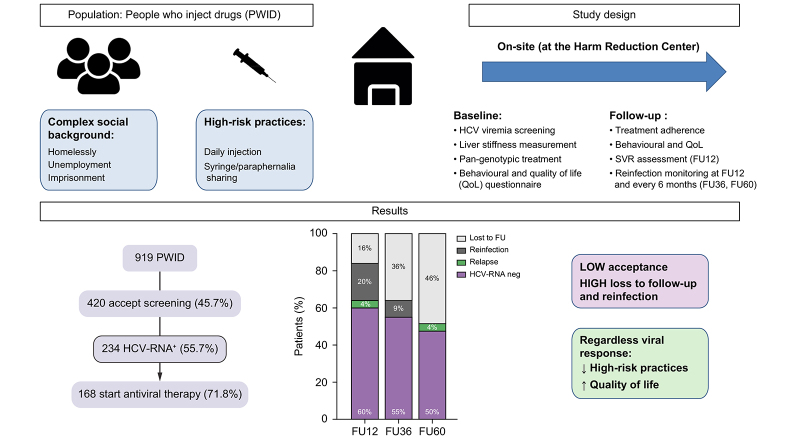
BACKGROUND & AIMS: Significant scale-up of treatment among people who inject drugs (PWID) is crucial to achieve WHO HCV elimination targets. We explored the impact of on-site HCV diagnosis and treatment on PWID in an externalised hepatology clinic at the biggest harm reduction centre (HRC) in Barcelona attending to a marginalised PWID population with ongoing high-risk practices.
On-site HCV point-of-care testing was performed for diagnosis and treatment delivery. HCV-RNA was assessed at SVR12 (sustained virologic response at 12 weeks) and every 6 months. The programme included behavioural questionnaires at baseline and after treatment.
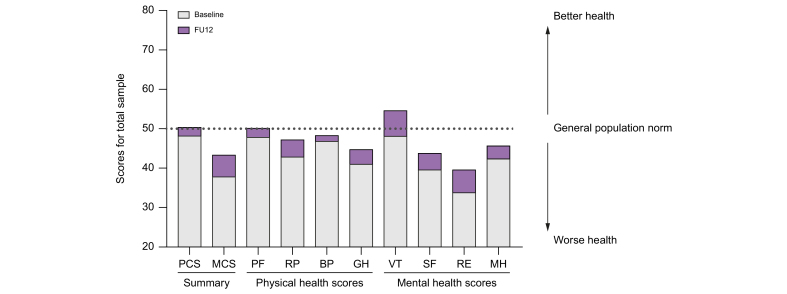
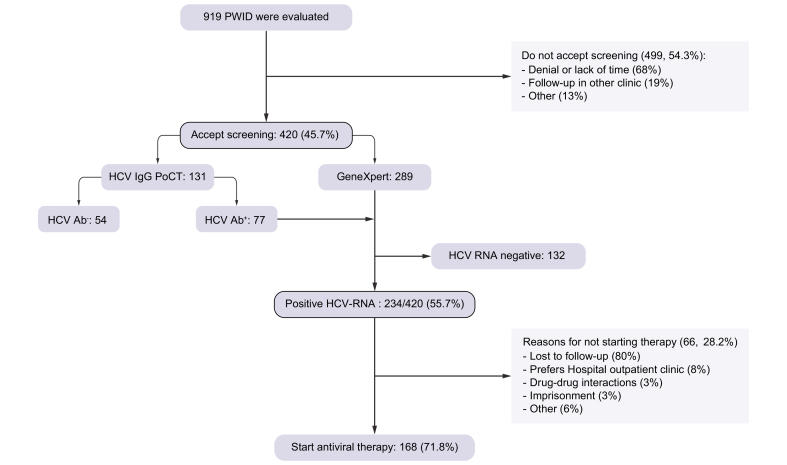
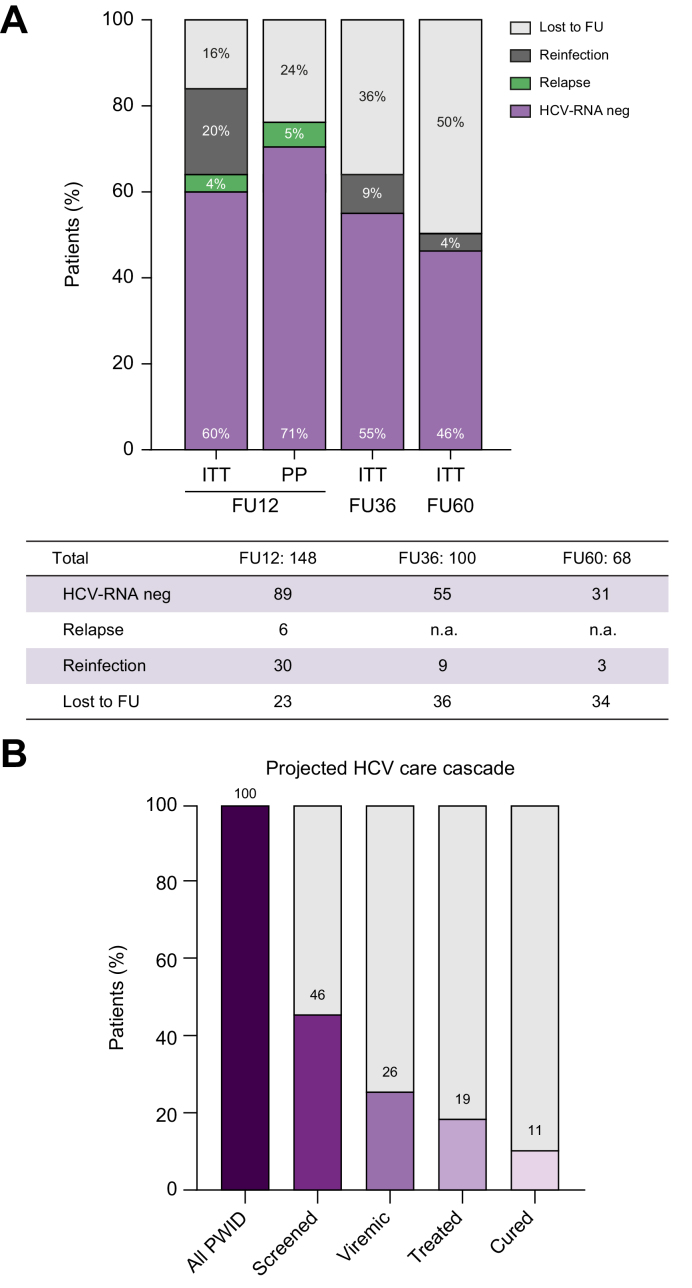
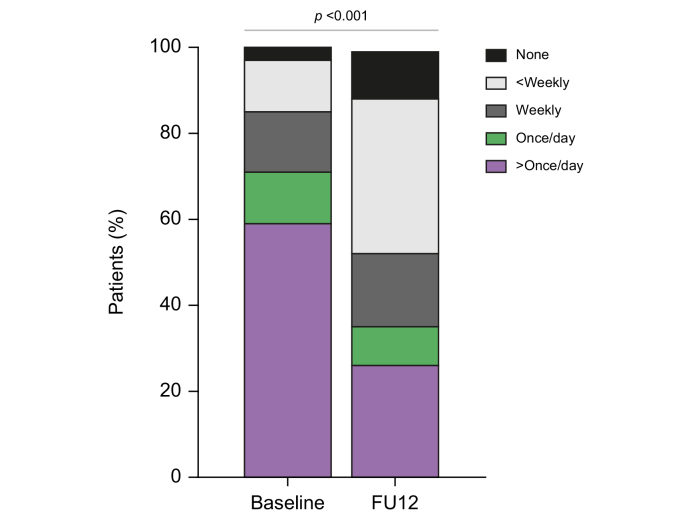
Between 2018 and 2020, 919 individuals were prospectively enrolled. Of these, only 46% accepted HCV screening. HCV-RNA+ prevalence was 55.7% (n = 234). Of the 168 (72%) individuals starting treatment, 48% were foreigners, 32% homeless, 73% unemployed, and 62% had a history of incarceration. At enrolment, 70% injected drugs daily and 30% reported sharing needles or paraphernalia. Intention-to-treat SVR12 was 60%; only 4% were virological failures, the remaining were either early reinfections (20%) or losses to follow-up (16%). The overall reinfection rate during follow-up was 31/100 persons/year. HIV coinfection and daily injection were associated with a higher risk of reinfection. Nonetheless, beyond viral clearance, antiviral therapy was associated with a significant reduction in injection frequency, risk practices, and homelessness.
HCV treatment can be successfully delivered to active PWID with high-risk practices and has a significant benefit beyond HCV elimination. However, approaching this difficult spectrum of the PWID population implies significant barriers such as low rate of screening acceptance and high dropout and reinfection rates.
People who inject drugs attending harm reduction centres represent the most difficult population to treat for hepatitis C. We show that hepatitis C treatment has a significant benefit beyond viral cure, including improving quality of life, and decreasing injection frequency and risk practices. However, intrinsic barriers and the high reinfection rates hamper the achievement of viral microelimination in this setting.
大幅扩大对注射吸毒者(PWID)的治疗对于实现世界卫生组织的丙型肝炎消除目标至关重要。我们在巴塞罗那最大的减少伤害中心(HRC)的一家外部肝病诊所,探讨了现场丙型肝炎诊断和治疗对PWID的影响,该诊所服务于有持续高风险行为的边缘化PWID人群。
进行现场即时丙型肝炎检测以进行诊断和治疗。在治疗12周时(SVR12,即持续病毒学应答)及之后每6个月评估丙型肝炎病毒核糖核酸(HCV-RNA)。该项目包括在基线和治疗后进行行为问卷调查。
2018年至2020年期间,前瞻性纳入了919人。其中,只有46%的人接受了丙型肝炎筛查。HCV-RNA阳性率为55.7%(n = 234)。在开始治疗的168人(72%)中,48%是外国人,32%无家可归,73%失业,62%有监禁史。在入组时,70%的人每天注射毒品,30%的人报告共用针头或用具。意向性治疗的SVR12为60%;只有4%是病毒学失败,其余的要么是早期再感染(20%),要么是失访(16%)。随访期间的总体再感染率为31/100人/年。合并感染艾滋病毒和每天注射与更高的再感染风险相关。尽管如此,除了病毒清除外,抗病毒治疗还与注射频率、风险行为和无家可归情况的显著减少相关。
丙型肝炎治疗可以成功地提供给有高风险行为的活跃PWID,并且除了消除丙型肝炎外还有显著益处。然而,接触这一困难的PWID人群存在重大障碍,如筛查接受率低、高辍学率和再感染率。
在减少伤害中心就诊的注射吸毒者是最难治疗丙型肝炎的人群。我们表明,丙型肝炎治疗除了病毒治愈外还有显著益处,包括改善生活质量、降低注射频率和风险行为。然而,内在障碍和高再感染率阻碍了在这种情况下实现病毒微消除。