African Centre of Excellence in the Prevention and Control of Communicable Diseases, University of Conakry, Conakry, Guinea.
Ministry of Health, Centre National de Formation et de Recherche en Santé Rurale de Maferinyah, Forécariah, Guinea.
Front Public Health. 2022 Oct 17;10:879850. doi: 10.3389/fpubh.2022.879850. eCollection 2022.
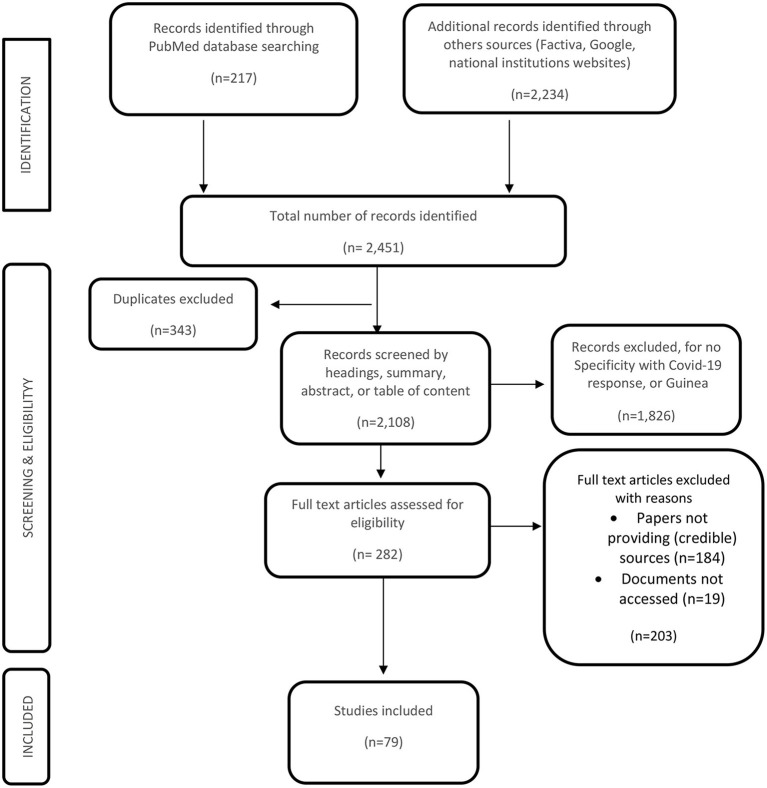
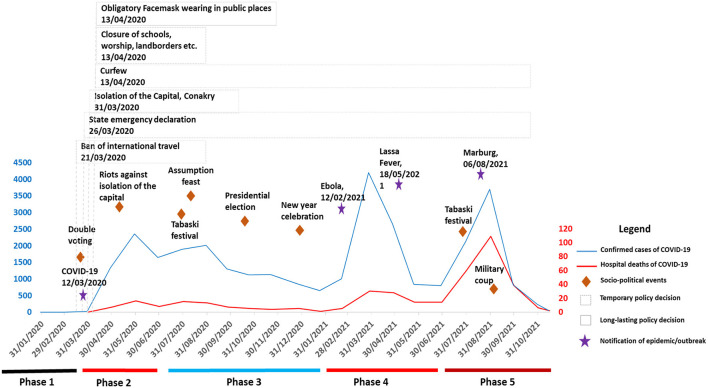
The outbreak of the novel coronavirus (SARS-CoV-2) in December 2019 prompted a response from health systems of countries across the globe. The first case of COVID-19 in Guinea was notified on 12 March 2020; however, from January 2020 preparations at policy and implementation preparedness levels had already begun. This study aimed to assess the response triggered in Guinea between 27 January 2020 and 1 November 2021 and lessons for future pandemic preparedness and response. We conducted a scoping review using three main data sources: policy documents, research papers and media content. For each of these data sources, a specific search strategy was applied, respectively national websites, PubMed and the Factiva media database. A content analysis was conducted to assess the information found. We found that between January 2020 and November 2021, the response to the COVID-19 pandemic can be divided into five phases: (1) anticipation of the response, (2) a sudden boost of political actions with the implementation of strict restrictive measures, (3) alleviation of restrictive measures, (4) multiple epidemics period and (5) the COVID-19 variants phase, including the strengthening of vaccination activities. This study provides several learning points for countries with similar contexts including: (1) the necessity of setting up, in the pre-epidemic period, an epidemic governance framework that is articulated with the country's health system and epidemiological contexts; (2) the importance of mobilizing, during pre-epidemic period, emergency funds for a rapid health system response whenever epidemics hit; (3) each epidemic is a new experience as previous exposure to similar ones does not necessarily guarantee population and health system resilience; (4) epidemics generate social distress because of the restrictive measures they require for their control, but their excessive securitization is counterproductive. Finally, from a political point of view, decision-making for epidemic control is not always disinterested; it is sometimes rooted in political computations, and health system actors should learn to cope with it while, at the same time, safeguarding trusted and efficient health system responses. We conclude that health system actors anticipated the response to the COVID-19 pandemic and (re-) adapted response strategies as the pandemic evolved in the country. There is a need to rethink epidemics governance and funding mechanisms in Guinea to improve the health system response to epidemics.
2019 年 12 月新型冠状病毒(SARS-CoV-2)的爆发促使全球各国的卫生系统做出反应。2020 年 3 月 12 日,几内亚通报了首例 COVID-19 病例;然而,从 2020 年 1 月开始,政策和实施准备层面的准备工作已经开始。本研究旨在评估 2020 年 1 月 27 日至 2021 年 11 月 1 日期间在几内亚引发的应对措施,以及为未来的大流行防范和应对提供经验教训。我们使用三个主要数据源进行了范围界定审查:政策文件、研究论文和媒体内容。对于每个这些数据源,分别应用了特定的搜索策略,即国家网站、PubMed 和 Factiva 媒体数据库。我们进行了内容分析以评估所发现的信息。我们发现,在 2020 年 1 月至 2021 年 11 月期间,对 COVID-19 大流行的应对可以分为五个阶段:(1)应对的预期,(2)突然增强政治行动,实施严格的限制措施,(3)缓解限制措施,(4)多疫情期,(5)COVID-19 变体阶段,包括加强疫苗接种活动。本研究为具有类似背景的国家提供了一些经验教训,包括:(1)有必要在大流行前建立一个与国家卫生系统和流行病学背景相衔接的流行治理框架;(2)在大流行前时期,为快速应对卫生系统,紧急筹集资金的重要性;(3)每次疫情都是新的体验,因为以前类似的经历并不能保证人口和卫生系统的弹性;(4)由于控制疫情需要采取限制措施,疫情会造成社会痛苦,但对其过度安全化会适得其反。最后,从政治角度来看,控制疫情的决策并不总是无私的;它有时植根于政治计算,卫生系统行为者应该学会应对,同时维护值得信赖和高效的卫生系统应对措施。我们的结论是,卫生系统行为者预期了 COVID-19 大流行的应对措施,并随着大流行在该国的发展,(重新)调整了应对策略。有必要重新思考几内亚的大流行治理和供资机制,以改善卫生系统对大流行的应对。