Department of Surgery, Amsterdam UMC, location University of Amsterdam, Amsterdam, the Netherlands.
Department of Pathology, Amsterdam UMC, location University of Amsterdam, Amsterdam, the Netherlands.
Br J Surg. 2022 Dec 13;110(1):67-75. doi: 10.1093/bjs/znac350.
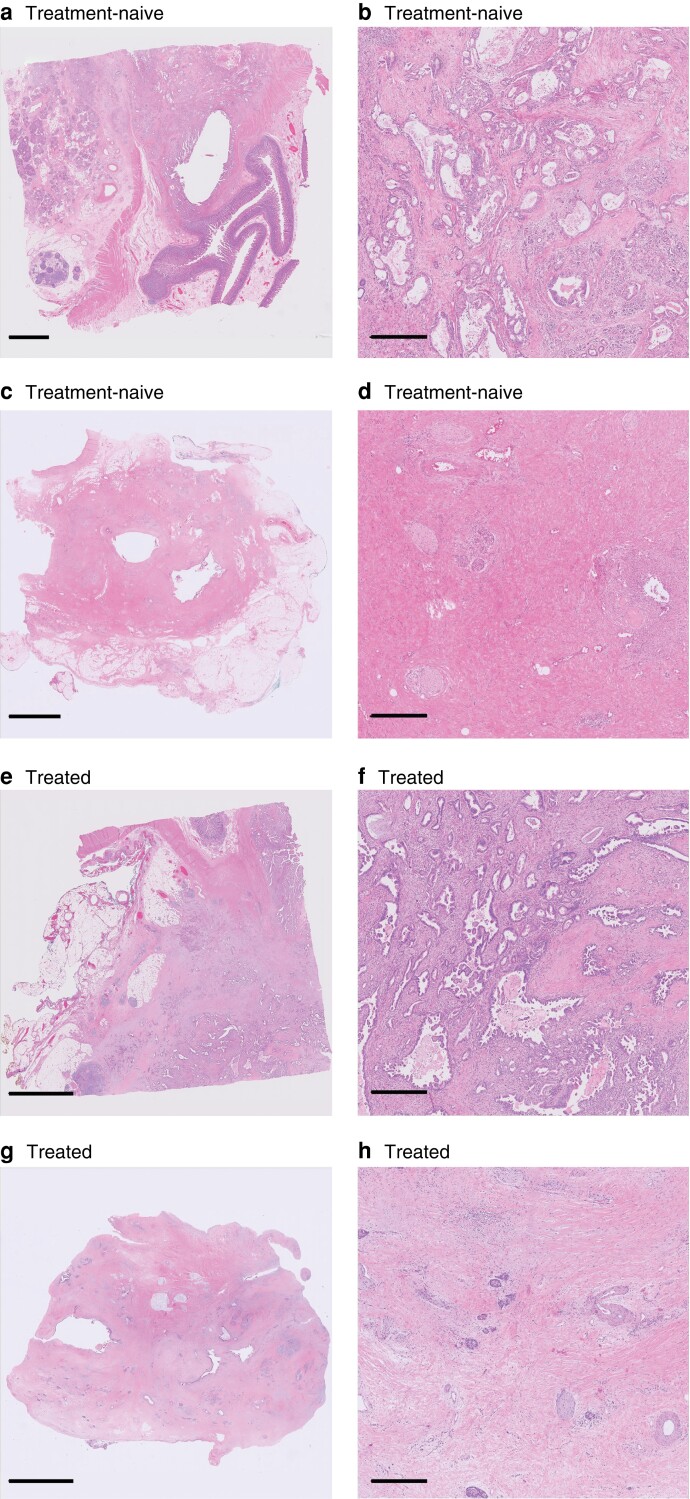
Most tumour response scoring systems for resected pancreatic cancer after neoadjuvant therapy score tumour regression. However, whether treatment-induced changes, including tumour regression, can be identified reliably on haematoxylin and eosin-stained slides remains unclear. Moreover, no large study of the interobserver agreement of current tumour response scoring systems for pancreatic cancer exists. This study aimed to investigate whether gastrointestinal/pancreatic pathologists can reliably identify treatment effect on tumour by histology, and to determine the interobserver agreement for current tumour response scoring systems.
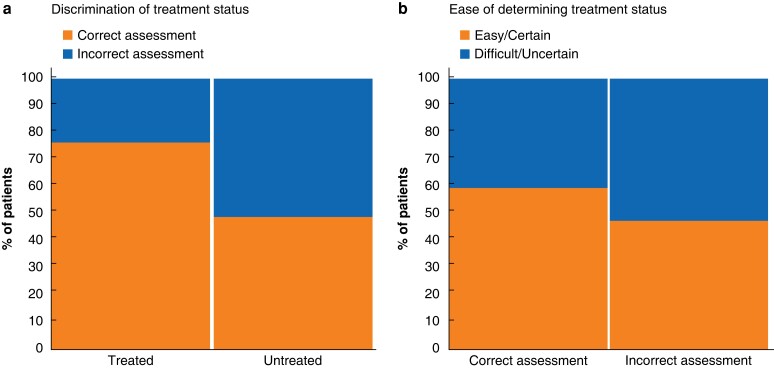
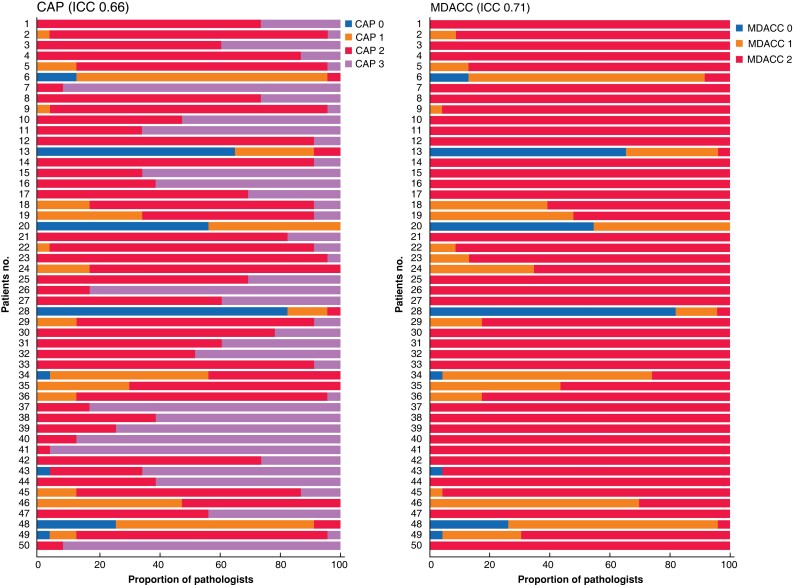
Overall, 23 gastrointestinal/pancreatic pathologists reviewed digital haematoxylin and eosin-stained slides of pancreatic cancer or treated tumour bed. The accuracy in identifying the treatment effect was investigated in 60 patients (30 treatment-naive, 30 after neoadjuvant therapy (NAT)). The interobserver agreement for the College of American Pathologists (CAP) and MD Anderson Cancer Center (MDACC) tumour response scoring systems was assessed in 50 patients using intraclass correlation coefficients (ICCs). An ICC value below 0.50 indicated poor reliability, 0.50 or more and less than 0.75 indicated moderate reliability, 0.75 or more and below 0.90 indicated good reliability, and above 0.90 indicated excellent reliability.
The sensitivity and specificity for identifying NAT effect were 76.2 and 49.0 per cent respectively. After NAT in 50 patients, ICC values for both tumour response scoring systems were moderate: 0.66 for CAP and 0.71 for MDACC.
Identification of the effect of NAT in resected pancreatic cancer proved unreliable, and interobserver agreement for the current tumour response scoring systems was suboptimal. These findings support the recently published International Study Group of Pancreatic Pathologists recommendations to score residual tumour burden rather than tumour regression after NAT.
大多数新辅助治疗后切除的胰腺癌肿瘤反应评分系统都对肿瘤退缩进行评分。然而,在苏木精和伊红染色切片上是否能可靠地识别治疗诱导的变化,包括肿瘤退缩,目前仍不清楚。此外,目前还没有关于胰腺癌肿瘤反应评分系统的观察者间一致性的大型研究。本研究旨在探讨胃肠/胰腺病理学家是否能够通过组织学可靠地识别治疗效果,并确定当前肿瘤反应评分系统的观察者间一致性。
共有 23 名胃肠/胰腺病理学家对胰腺癌或治疗后的肿瘤床的数字苏木精和伊红染色切片进行了回顾。在 60 名患者(30 名治疗前,30 名新辅助治疗后)中研究了识别治疗效果的准确性。使用组内相关系数(ICC)评估 50 名患者中美国病理学家学院(CAP)和 MD 安德森癌症中心(MDACC)肿瘤反应评分系统的观察者间一致性。ICC 值低于 0.50 表示可靠性差,0.50 或更高但低于 0.75 表示中等可靠性,0.75 或更高但低于 0.90 表示良好可靠性,高于 0.90 表示极好的可靠性。
识别 NAT 效果的敏感性和特异性分别为 76.2%和 49.0%。在 50 名接受新辅助治疗的患者中,两种肿瘤反应评分系统的 ICC 值均为中等:CAP 为 0.66,MDACC 为 0.71。
在切除的胰腺癌中,NAT 效果的识别不可靠,目前肿瘤反应评分系统的观察者间一致性不理想。这些发现支持最近发表的国际胰腺病理学家研究组的建议,即对 NAT 后残留肿瘤负担而不是肿瘤退缩进行评分。