Surgo Ventures, Washington, DC, USA.
Department of Community Health Sciences, University of Manitoba, Winnipeg, Canada.
Glob Health Sci Pract. 2022 Jun 29;10(3). doi: 10.9745/GHSP-D-21-00413.
Although community health workers (CHWs) are effective at mobilizing important health behaviors, there is limited evidence on how financial incentive systems can best be designed to drive their effectiveness. This study intends to bridge this evidence gap by analyzing the compensation model of India's accredited social health activist (ASHA) program and identifying areas of improvement in the system's design and implementation.
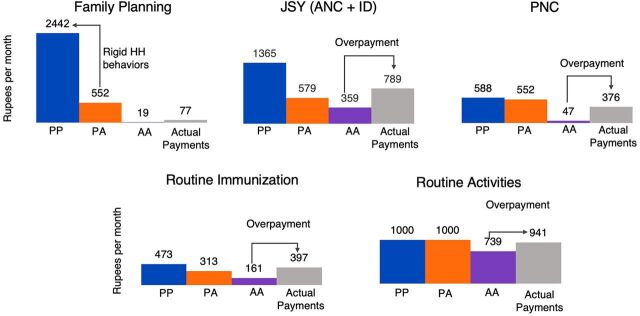
We analyze the ASHA program in Uttar Pradesh, India. ASHAs receive compensation through a mix of program-linked, performance-based, and routine activity-based incentive structures. Using multiple data sources, including a novel linked household and ASHA survey, we estimate ASHA performance-linked incentive earnings under different scenarios of ASHA actions and household behaviors. Juxtaposing statistical projection models and actual government payments, we identified which incentives promised the highest payments, which were claimed or not, which could be claimed more by increasing ASHA actions, and which were paid despite not meeting payment criteria. We also report findings on ASHA awareness of and experiences with claiming incentives.
We find crucial gaps and implementation challenges in the ASHA incentive structure. ASHAs could double their earnings by completing certain tasks within their control. ASHAs may also be paid for partial completion of activities, as incentives are paid in lump sums for a series of activities rather than for each activity. Family planning incentives have the largest gap between potential and actual earnings. Incentivizing ASHAs for achieving certain health outcomes is inefficient, as no clear linkage was found between the achievability of such health outcomes and the claim amounts.
There are several opportunities for improving CHW compensation, from improving the incentive claims process to shifting focus to achievable outcomes. Optimizing incentive system designs can further enhance CHW effectiveness globally to affect key health behaviors.
尽管社区卫生工作者(CHWs)在调动重要健康行为方面非常有效,但关于如何设计最佳财务激励系统以提高其效果的证据有限。本研究旨在通过分析印度认证社会卫生活动家(ASHA)计划的薪酬模式,并确定系统设计和实施中需要改进的领域,来填补这一证据空白。
我们分析了印度北方邦的 ASHA 计划。ASHA 通过项目相关的、基于绩效的和常规活动的混合激励结构获得报酬。我们使用包括一项新颖的家庭和 ASHA 调查在内的多个数据源,根据 ASHA 行动和家庭行为的不同情景,估计 ASHA 绩效相关激励收入。通过将统计预测模型与实际政府支付进行对比,我们确定了哪些激励措施承诺支付最高的报酬,哪些被承诺但未兑现,哪些可以通过增加 ASHA 行动来增加报酬,以及哪些即使未达到支付标准也得到了支付。我们还报告了 ASHA 对激励措施的认识和实施经验的调查结果。
我们发现 ASHA 激励结构存在重大差距和实施挑战。ASHA 通过完成其可控范围内的某些任务,可以将收入增加一倍。激励措施还可以按部分完成活动支付报酬,因为激励措施是按一系列活动的总额支付的,而不是每项活动都支付。计划生育激励措施的潜在收入和实际收入之间存在最大差距。激励 ASHA 实现某些健康结果的效率不高,因为没有发现这些健康结果的可实现性与索赔金额之间的明确联系。
从改善激励索赔流程到将重点转移到可实现的结果,都有几种改进 CHW 薪酬的机会。优化激励系统设计可以进一步提高全球 CHW 的效果,从而影响关键健康行为。