School of Health Sciences, Faculty of Medicine and Health, University of New South Wales, High St, Kensington, NSW, 2052, Australia.
Centre for Pain IMPACT, Neuroscience Research Australia, Barker St, Randwick, NSW, 2031, Australia.
BMC Med Res Methodol. 2022 Nov 4;22(1):285. doi: 10.1186/s12874-022-01763-x.
Meta-analyses of analgesic medicines for low back pain often rescale measures of pain intensity to use mean difference (MD) instead of standardised mean difference for pooled estimates. Although this improves clinical interpretability, it is not clear whether this method is justified. Our study evaluated the justification for this method.
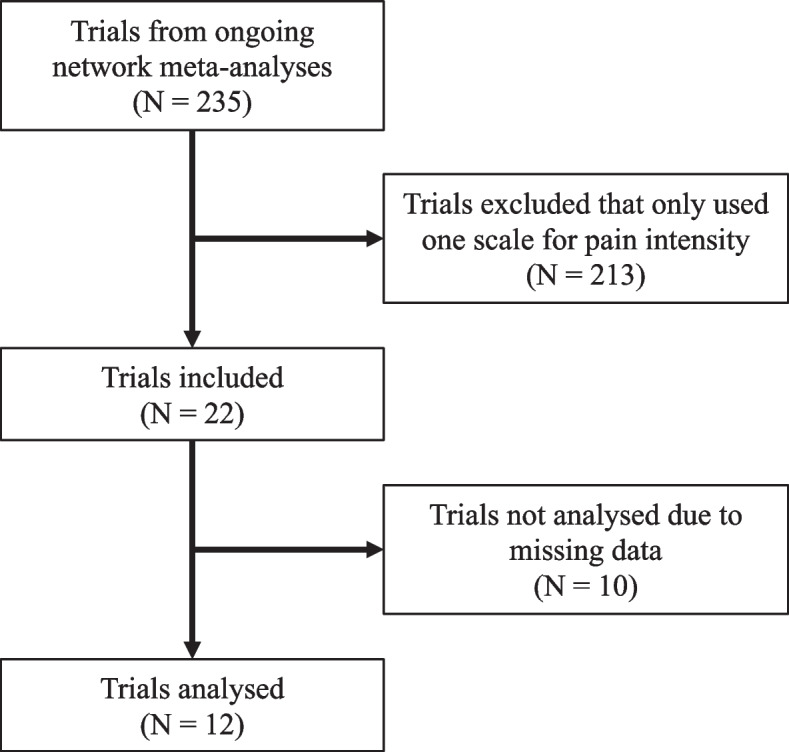
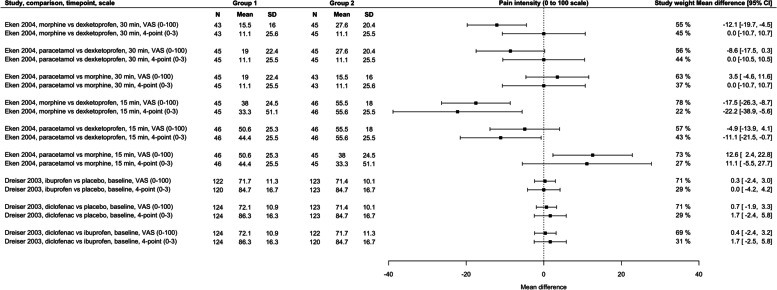
We identified randomised clinical trials of analgesic medicines for adults with low back pain that used two scales with different ranges to measure the same construct of pain intensity. We transformed all data to a 0-100 scale, then compared between-group estimates across pairs of scales with different ranges.
Twelve trials were included. Overall, differences in means between pain intensity measures that were rescaled to a common 0-100 scale appeared to be small and randomly distributed. For one study that measured pain intensity on a 0-100 scale and a 0-10 scale; when rescaled to 0-100, the difference in MD between the scales was 0.8 points out of 100. For three studies that measured pain intensity on a 0-10 scale and 0-3 scale; when rescaled to 0-100, the average difference in MD between the scales was 0.2 points out of 100 (range 5.5 points lower to 2.7 points higher). For two studies that measured pain intensity on a 0-100 scale and a 0-3 scale; when rescaled to 0-100, the average difference in MD between the scales was 0.7 points out of 100 (range 6.2 points lower to 12.1 points higher). Finally, for six studies that measured pain intensity on a 0-100 scale and a 0-4 scale; when rescaled to 0-100, the average difference in MD between the scales was 0.7 points (range 5.4 points lower to 8.3 points higher).
Rescaling pain intensity measures may be justified in meta-analyses of analgesic medicines for low back pain. Systematic reviewers may consider this method to improve clinical interpretability and enable more data to be included.
STUDY REGISTRATION/DATA AVAILABILITY: Open Science Framework (osf.io/8rq7f).
对用于治疗腰痛的镇痛药物进行的荟萃分析通常会重新调整疼痛强度测量值,以使用均数差值 (MD) 代替汇总估计值的标准化均数差值。虽然这提高了临床可解释性,但尚不清楚这种方法是否合理。我们的研究评估了这种方法的合理性。
我们确定了针对腰痛成人使用两种具有不同范围的镇痛药物的随机临床试验,以测量相同的疼痛强度结构。我们将所有数据转换为 0-100 量表,然后比较具有不同范围的量表之间的组间估计值。
共纳入 12 项试验。总体而言,重新调整为共同的 0-100 量表的疼痛强度测量值之间的均值差异似乎很小且随机分布。对于一项在 0-100 量表和 0-10 量表上测量疼痛强度的研究;当重新调整为 0-100 时,两个量表之间 MD 的差异为 100 分中的 8 分。对于三项在 0-10 量表和 0-3 量表上测量疼痛强度的研究;当重新调整为 0-100 时,两个量表之间 MD 的平均差异为 100 分中的 0.2 分(范围低 5.5 分至高 2.7 分)。对于两项在 0-100 量表和 0-3 量表上测量疼痛强度的研究;当重新调整为 0-100 时,两个量表之间 MD 的平均差异为 100 分中的 0.7 分(范围低 6.2 分至高 12.1 分)。最后,对于六项在 0-100 量表和 0-4 量表上测量疼痛强度的研究;当重新调整为 0-100 时,两个量表之间 MD 的平均差异为 0.7 分(范围低 5.4 分至高 8.3 分)。
在治疗腰痛的镇痛药物的荟萃分析中,重新调整疼痛强度测量值可能是合理的。系统评价者可以考虑使用这种方法来提高临床可解释性,并使更多的数据能够被纳入。
研究注册/数据可用性:开放科学框架(osf.io/8rq7f)。