Prenatal diagnosis department, Chengdu Women's and Children's Central Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, China.
BMC Pregnancy Childbirth. 2022 Nov 4;22(1):813. doi: 10.1186/s12884-022-05139-3.
Down syndrome (DS) is the most common congenital cause of intellectual disability and also leads to numerous metabolic and structural problems. This study aims to explore the application value of chromosomal microarray analysis (CMA) and karyotyping in prenatal diagnosis for pregnant women with abnormal DS screening results.
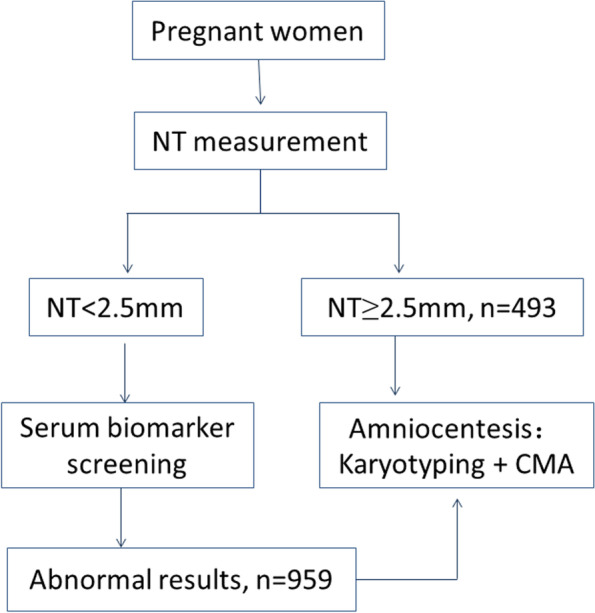
The study recruited 1452 pregnant women with abnormal DS screening results including 493 with an enlarged nuchal translucency thickness (NT ≥ 2.5 mm) and 959 with an abnormal second-trimester maternal serum biomarker screening results. They underwent amniocentesis to obtain amniotic fluid for CMA and karyotyping.
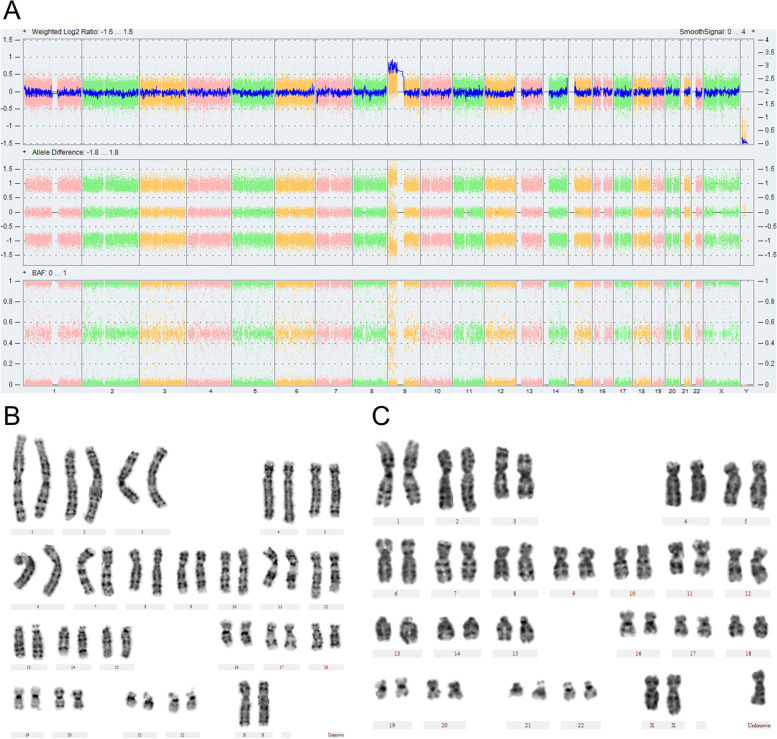
CMA identified 74/1452 abnormal results, which was more efficient than karyotyping (51/1452, P < 0.05.) CMA is equivalent to traditional karyotyping for identifying aneuploidies. Compared to karyotyping CMA identified 1.90% more copy number variants (CNVs) ranging from 159Kb to 6496Kb. However, 34.4% of them were recurrent pathogenic CNVs associated with risk of neurodevelopmental disorders. CMA identified 13 variants of uncertain significance (VUS) results and 1 maternal uniparental disomy (UPD) of chromosome 7. Karyotyping identified 3 mosaic sex chromosome aneuploidy and 4 balanced translocation which could not be identified by CMA. In enlarged NT group, karyotyping identified 80.9% abnormal results while in serum screening group karyotyping identified 35.7%. However, the incidence of pathogenic/likely pathogenic (P/LP) CNVs was nearly the same in both groups. That was because aneuploidies and gross duplication/deletion were previously screened out by NT scan.
CMA and karyotyping have both advantages and disadvantages in prenatal diagnosis of pregnant women with abnormal DS screening results. However, there was not enough evidence to support routine CMA in pregnant women with abnormal DS screening results.
唐氏综合征(DS)是最常见的先天性智力障碍病因,同时还会导致多种代谢和结构问题。本研究旨在探讨染色体微阵列分析(CMA)和核型分析在唐氏综合征筛查异常孕妇产前诊断中的应用价值。
本研究共纳入 1452 例唐氏综合征筛查异常孕妇,其中 493 例颈项透明层(NT)增厚(NT≥2.5mm),959 例孕中期母血清学标志物筛查异常。所有孕妇均接受羊膜穿刺术以获取羊水进行 CMA 和核型分析。
CMA 共检出 74/1452 例异常结果,其检出效率高于核型分析(51/1452,P<0.05)。CMA 与传统核型分析在识别非整倍体方面具有等效性。与核型分析相比,CMA 多检出 1.90%(159Kb 至 6496Kb)拷贝数变异(CNV)。然而,其中 34.4%为与神经发育障碍风险相关的常见致病性 CNV。CMA 还检出 13 例意义未明的变异(VUS)结果和 1 例 7 号染色体单亲二体(UPD)。核型分析检出 3 例性染色体嵌合型非整倍体和 4 例 CMA 无法识别的平衡易位。在 NT 增厚组,核型分析检出 80.9%的异常结果,而在血清学筛查组仅检出 35.7%。然而,两组致病性/可能致病性(P/LP)CNV 的发生率相近。这是因为 NT 扫描已排除了非整倍体和大片段重复/缺失。
CMA 和核型分析在唐氏综合征筛查异常孕妇的产前诊断中各有优势和不足。然而,目前尚无足够证据支持对唐氏综合征筛查异常孕妇常规进行 CMA。