Huntsman Cancer Institute, University of Utah, 2000 Cir of Hope Dr, Salt Lake City, UT, 84112, USA.
University of Utah Intermountain Healthcare Department of Population Health Sciences, School of Medicine, University of Utah, 295 Chipeta Way, Salt Lake City, UT, 84108, USA.
BMC Womens Health. 2022 Nov 4;22(1):430. doi: 10.1186/s12905-022-02016-1.
Ovarian cancer is often diagnosed at a late stage, when survival is poor. Qualitative narratives of patients' pathways to ovarian cancer diagnoses may identify opportunities for earlier cancer detection and, consequently, earlier stage at diagnosis.
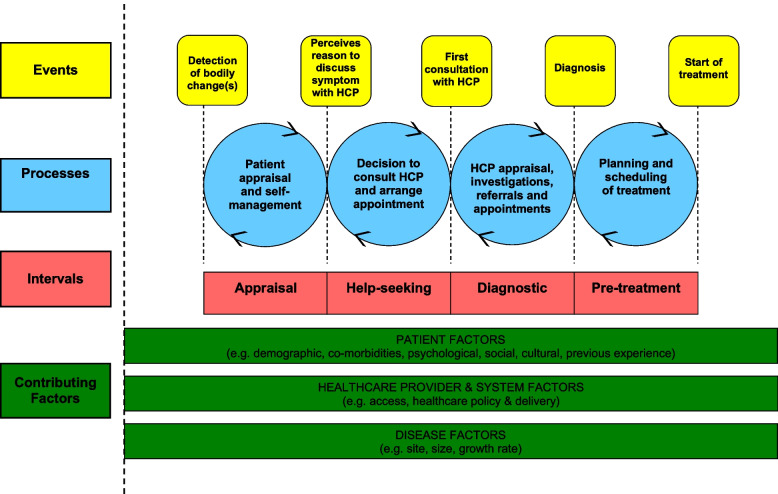
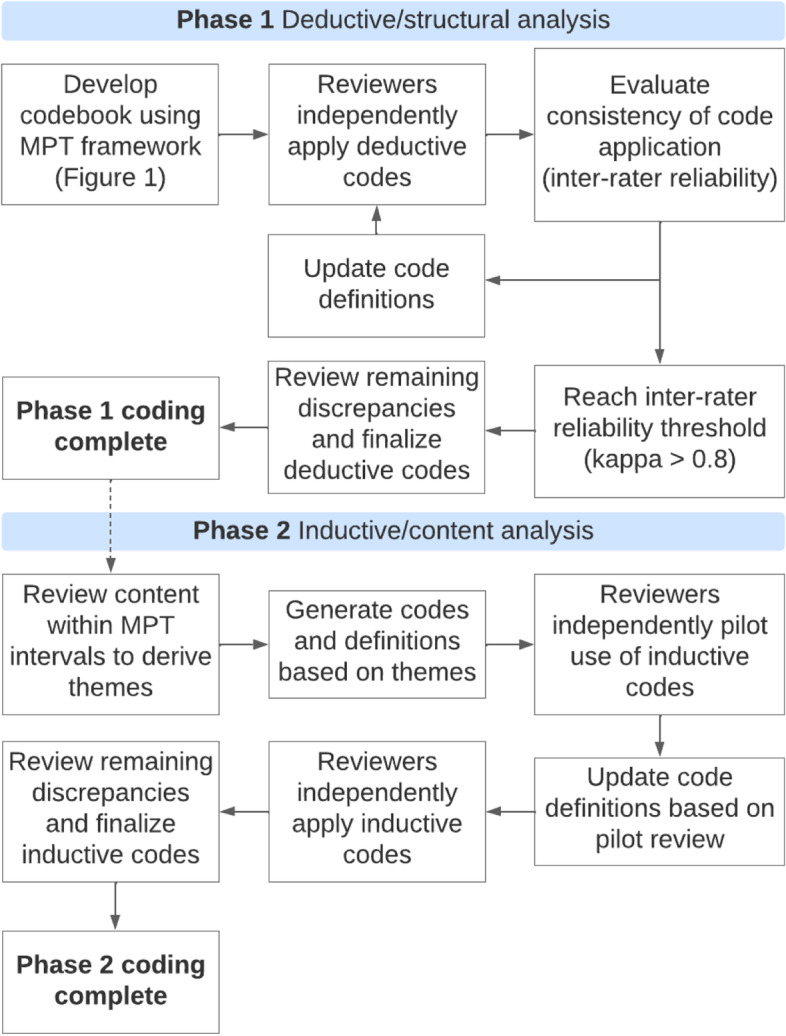
We conducted semi-structured interviews of ovarian cancer patients and survivors (n = 14) and healthcare providers (n = 11) between 10/2019 and 10/2021. Interviews focused on the time leading up to an ovarian cancer diagnosis. Thematic analysis was conducted by two independent reviewers using a two-phase deductive and inductive coding approach. Deductive coding used a priori time intervals from the validated Model of Pathways to Treatment (MPT), including self-appraisal and management of symptoms, medical help-seeking, diagnosis, and pre-treatment. Inductive coding identified common themes within each stage of the MPT across patient and provider interviews.
The median age at ovarian cancer diagnosis was 61.5 years (range, 29-78 years), and the majority of participants (11/14) were diagnosed with advanced-stage disease. The median time from first symptom to initiation of treatment was 2.8 months (range, 19 days to 4.7 years). The appraisal and help-seeking intervals contributed the greatest delays in time-to-diagnosis for ovarian cancer. Nonspecific symptoms, perceptions of health and aging, avoidant coping strategies, symptom embarrassment, and concerns about potential judgment from providers prolonged the appraisal and help-seeking intervals. Patients and providers also emphasized access to care, including financial access, as critical to a timely diagnosis.
Interventions are urgently needed to reduce ovarian cancer morbidity and mortality. Population-level screening remains unlikely to improve ovarian cancer survival, but findings from our study suggest that developing interventions to improve self-appraisal of symptoms and reduce barriers to help-seeking could reduce time-to-diagnosis for ovarian cancer. Affordability of care and insurance may be particularly important for ovarian cancer patients diagnosed in the United States.
卵巢癌通常在晚期诊断,此时生存率较差。对患者卵巢癌诊断途径的定性叙述可能会发现更早发现癌症的机会,从而更早发现癌症。
我们在 2019 年 10 月至 2021 年 10 月期间对卵巢癌患者和幸存者(n=14)以及医疗保健提供者(n=11)进行了半结构化访谈。访谈重点是卵巢癌诊断前的时间。两位独立审查员使用两阶段演绎和归纳编码方法进行主题分析。演绎编码使用了验证后的治疗途径模型(MPT)的预先确定的时间间隔,包括自我评估和症状管理、寻求医疗帮助、诊断和治疗前。归纳编码在患者和提供者访谈中识别了 MPT 各个阶段的常见主题。
卵巢癌诊断的中位年龄为 61.5 岁(范围为 29-78 岁),大多数参与者(11/14)被诊断为晚期疾病。从首次出现症状到开始治疗的中位时间为 2.8 个月(范围为 19 天至 4.7 年)。评估和寻求帮助的间隔对卵巢癌的诊断时间延迟贡献最大。非特异性症状、对健康和衰老的看法、回避应对策略、症状尴尬以及对提供者潜在判断的担忧延长了评估和寻求帮助的间隔。患者和提供者还强调了获得医疗保健的机会,包括经济机会,这对及时诊断至关重要。
迫切需要采取干预措施来降低卵巢癌的发病率和死亡率。人群筛查仍不太可能改善卵巢癌的生存率,但我们的研究结果表明,开发改善自我评估症状和减少寻求帮助障碍的干预措施可以减少卵巢癌的诊断时间。在美国,获得医疗保健的可负担性和保险可能对被诊断为卵巢癌的患者尤为重要。